







Why this topic is harder than headlines suggest
Cannabis is more socially accepted than it was a decade ago. In many U.S. states, adults can legally use it. That shift has changed how people talk about risk. It has not changed a basic fact of medicine: pregnancy and breastfeeding are treated as distinct exposure settings because another developing body is involved, and because clinicians are asked to make decisions before certainty arrives.
That is the tension that most headlines flatten. Some coverage treats any cannabis use in pregnancy as settled proof of severe harm. Other coverage leans on gaps in the data and implies there is little to worry about. Neither framing is good enough. The actual picture is messier, and more consequential, because it sits at the intersection of pharmacology, observational research, prenatal care, substance-use stigma, and state power.
Use during pregnancy is not rare. SAMHSA reported in 2020 that among pregnant women ages 15 to 44, past-month marijuana use was 3.0% overall, rising to 5.7% in the first trimester, then falling to 3.3% in the second and 1.8% in the third. Those numbers likely miss some use because self-report is an imperfect method when patients fear judgment, reporting requirements, or legal fallout. At the same time, product strength has changed sharply over the years, so an older study on lower-potency cannabis does not map neatly onto current exposure.
Legalization for adults does not mean legal safety in pregnancy[1]Despite expanding cannabis legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use. STAT staff. STAT, 2026. https://www.statnews.com/2026/03/02/cannabis-laws-pregnancy-cps/
Legalization for nonpregnant adults has led many people to assume the legal risk is gone. It is not. STAT reported in 2026 that “despite expanding cannabis legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use.” That line matters because it cuts against a common public assumption: if a substance is legal for adult use, disclosing it to a clinician should be straightforward. In pregnancy, that can be dangerously wrong.
The legal landscape is fragmented. State laws differ on mandated reporting, newborn drug testing, neglect definitions, and whether prenatal substance exposure can trigger child welfare involvement. Hospital policies differ too. Screening practices are not applied evenly, and punitive responses have repeatedly fallen hardest on low-income patients and patients of color. The result is not just unfairness. It can also become a medical problem, because fear of being reported can push people away from prenatal care, substance-use treatment, and honest conversations about nausea, sleep, anxiety, or pain.[2]Marijuana Use During Pregnancy and Lactation. American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 722, 2017. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2017/10/marijuana-use-during-pregnancy-and-lactation
That is one reason public-health groups have emphasized non-punitive care even while advising against use. ACOG’s Committee Opinion No. 722, first issued in 2017 and reaffirmed in 2021, states that “women who are pregnant or contemplating pregnancy should be encouraged to discontinue marijuana use.” But ACOG has also argued that the goal of screening is treatment and support, not punishment. That distinction is easy to miss in public debate. Clinical guidance can be firm about avoiding exposure while also opposing carceral responses that make care worse.
Breastfeeding raises a related problem. Cannabis may be legal in a state, but THC does not stop at the label or statute. Delta-9-tetrahydrocannabinol is lipophilic, crosses the placenta, and is excreted into breast milk. The CDC states that “breast milk can contain THC for up to 6 days after use, according to one study. Other studies have noted even longer duration.” A legal market does not erase that exposure pathway.
Why the evidence sounds contradictory
The short version is simple: there are reasons for concern, but much of the research is observational and hard to interpret cleanly. That creates a situation where associations can be real, clinically relevant, and still not provide tidy causal estimates.
THC crosses the placenta.Strong evidence
[3]Cannabis and Pregnancy. Centers for Disease Control and Prevention. CDC, 2024. https://www.cdc.gov/cannabis/health-effects/pregnancy.htmlStart with what is biologically plausible. THC crosses the placenta. The fetal brain develops over a long period and uses endogenous cannabinoid signaling as part of normal neurodevelopment. That does not prove a specific outcome from every level of exposure, but it gives researchers a credible mechanism for concern. The CDC puts it plainly: “The chemicals in cannabis (in particular, tetrahydrocannabinol or THC) pass through your system to your baby and may harm your baby’s development.”
Prenatal cannabis exposure is associated with lower birth weight, and may also be associated with preterm birth and NICU admission.Limited evidence
Then move to the outcomes research. Across reviews and cohort studies, prenatal cannabis exposure has been linked with lower birth weight, and in some analyses with preterm birth and NICU admission. There are also signals in later childhood for attention, executive function, and behavior. But the signal is uneven. Some studies find associations that weaken after adjustment; others find effects only in some subgroups, exposure windows, or outcome measures.
Why the instability? Confounding is the biggest reason. People who use cannabis during pregnancy may also be more likely, on average, to use tobacco, alcohol, or other substances; to experience housing insecurity or chronic stress; or to have less access to prenatal care. Those factors matter on their own. Older studies also reflect very different THC concentrations than current products, and many rely on self-report rather than toxicology. A patient using cannabis once for first-trimester nausea is not the same exposure case as daily use of high-potency concentrates, yet some datasets cannot sort that out.[4]Marijuana Use During Pregnancy and Breastfeeding: Implications for Neonatal and Childhood Outcomes. Seth D. Ammerman, Richard J. Ryan, Mary E. O'Connor, et al.. Pediatrics, 2018. https://publications.aap.org/pediatrics/article/142/3/e20181889/38625/Marijuana-Use-During-Pregnancy-and-Breastfeeding
Breastfeeding evidence is thinner still. ACOG says, “There are insufficient data to evaluate the effects of marijuana use on infants during lactation and breastfeeding, and in the absence of such data, marijuana use is discouraged.” The American Academy of Pediatrics said in 2018, “Data are insufficient to assess the effects of exposure of infants to maternal marijuana use during breastfeeding. As a result, maternal marijuana use while breastfeeding is discouraged.” That is not a claim of no risk. It is a statement that the evidence is limited while transfer to milk is established.
This is why a 2026 report could accurately say both that “the evidence on cannabis use in pregnancy remains mixed” and that new guidance warns against use during pregnancy because of potential fetal risks. Those statements are not inconsistent. They reflect different jobs. Researchers describe uncertainty. Clinicians must still advise patients when uncertainty involves a fetus or infant.
How this article will separate known risks from unknowns
How the article sorts the evidence
- Established exposure pathways
- THC reaches the fetus during pregnancy and appears in breast milk after maternal use.
- Consistent risk signals
- Lower birth weight is one of the more repeated findings; preterm birth, NICU admission, and later neurobehavioral differences remain concerning.
- Genuine unknowns
- Dose-response thresholds, product-specific effects, clinical impact of infant exposure through milk, and the amount of harm attributable to cannabis itself rather than correlated conditions.
This article will not treat every association as settled proof, and it will not pretend that missing data are reassuring. Instead it will sort findings into three buckets: established exposure pathways, consistent risk signals, and genuine unknowns.[5]Academy of Breastfeeding Medicine Clinical Protocol #21: Breastfeeding in the Setting of Substance Use and Substance Use Disorder. Academy of Breastfeeding Medicine. ABM Clinical Protocol, 2023. https://www.bfmed.org/protocols
Established exposure pathways come first. THC reaches the fetus during pregnancy and appears in breast milk after maternal use. That is not speculative. It is the basis for the caution shared by the CDC, ACOG, the AAP, and the Academy of Breastfeeding Medicine. ABM’s 2023 Protocol #21 says, “We encourage cessation and/or reduction of cannabis use during breastfeeding.” That wording reflects real-world care, where some patients will not stop immediately, but it does not endorse use as safe.
Next are the better-supported risk signals: lower birth weight is one of the more repeated findings, while preterm birth, NICU admission, and later neurobehavioral differences remain concerning but are harder to pin down with precision. Finally come the unknowns: dose-response thresholds, product-specific effects, how long infant exposure through milk matters clinically, and how much of the observed harm is due to cannabis itself rather than correlated conditions.
That approach matters because public-health guidance is often more definite than the research base. It has to be. When the stakes include fetal growth, infant exposure, and long-term neurodevelopment, “we are not fully sure” does not translate into “probably fine.”
What cannabis exposure means in pregnancy and lactation
| Exposure pattern | Why it matters clinically |
|---|---|
| Smoking dried flower | Combines cannabinoid exposure with combustion products; dose varies by inhalation behavior. |
| Vaping a cartridge | Rapid delivery to blood; absorbed dose depends on device, concentration, and puffing pattern. |
| Eating a THC edible | Slower onset and longer duration; labeled dose may not predict actual effect cleanly. |
| Swallowing an oil capsule | Oral route with first-pass metabolism and variable blood levels over time. |
| Taking a CBD tincture | May still contain THC or contaminants; not automatically safe in pregnancy. |
| Using a high-potency concentrate | Much higher THC exposure than older study eras often captured. |
| Using a product sold as hemp-derived | Label does not answer whether THC or other active cannabinoids are present at meaningful levels. |
“Cannabis exposure” sounds simple. It is not. In pregnancy and breastfeeding, that phrase can mean smoking dried flower, inhaling vapor from a cartridge, eating a THC edible, swallowing an oil capsule, taking a CBD tincture, using a high-potency concentrate, or using a product sold as hemp-derived. It can also mean cannabis used alone or mixed with nicotine in a blunt or spliff, which matters because tobacco exposure is itself tied to fetal growth restriction, preterm birth, and later respiratory risk. When studies treat all of these patterns as one thing, the result is a blurry evidence base.
That blur matters because clinical advice is stricter than the data are precise. ACOG’s Committee Opinion No. 722, issued in 2017 and reaffirmed in 2021, states that women who are pregnant or contemplating pregnancy should be encouraged to discontinue marijuana use. The CDC in 2024 said the chemicals in cannabis, “in particular, tetrahydrocannabinol or THC,” pass through the pregnant person’s system to the fetus and may harm development. The American Academy of Pediatrics took a similar line in 2018 for breastfeeding, and the Academy of Breastfeeding Medicine’s Protocol #21, revised in 2023, encourages cessation or reduction during lactation. Those recommendations are not based on perfect evidence. They are based on enough concern, and enough pharmacologic plausibility, to advise avoidance.[6]Despite expanding cannabis legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use. STAT staff. STAT, 2026. https://www.statnews.com/2026/03/02/cannabis-laws-pregnancy-cps/
At the same time, public discussion often skips a hard truth: legalization has not insulated pregnant people from punishment. STAT reported in 2026 that despite expanding legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use, even as “the evidence on cannabis use in pregnancy remains mixed.” That tension shapes how “exposure” is recorded, because patients may underreport use when disclosure can trigger surveillance.
THC, CBD, and whole-plant products are not the same question
The question most pregnancy studies answer is not “What does a 2025 live-resin vape with 82% THC do in the second trimester?” It is usually closer to “Did this patient report marijuana use at some point during pregnancy?” That is a much coarser question.
THC, or delta-9-tetrahydrocannabinol, is the main psychoactive cannabinoid and the one most clearly implicated in placental transfer and breast milk exposure. CBD, or cannabidiol, is pharmacologically different. It does not produce the same intoxication profile, but that does not make it automatically safe in pregnancy. CBD products vary widely in purity, may contain measurable THC, and may carry pesticides, heavy metals, solvents, or inaccurate labels. Whole-plant products add another layer because they contain dozens of cannabinoids and terpenes, and combustion adds toxic byproducts that are not specific to cannabis but still matter to fetal and infant exposure.
This is why “marijuana use” in older studies does not map neatly onto modern shelves. Potency has changed sharply over time. A joint studied in the 1990s was often far lower in THC than a contemporary concentrate, edible, or vape cartridge. Some products sold outside regulated systems are even less predictable. “Hemp-derived” also needs care as a label. Hemp products can contain CBD, delta-8 THC, delta-10 THC, or enough delta-9 THC to matter biologically, especially with repeated use. Calling something hemp does not answer the safety question in pregnancy.
Nor does “medical use.” Some pregnant patients self-treat nausea, vomiting, pain, anxiety, or insomnia with cannabis. Professional groups still advise against it. ACOG explicitly discourages recommending marijuana for medicinal purposes during preconception, pregnancy, and lactation because pregnancy-specific safety data are weak and alternatives exist. A 2026 industry press report described new guidance warning against cannabis use during pregnancy because of potential fetal risks. The source is not a clinical society statement by itself, but it reflects where mainstream guidance remains: avoid use, even if the patient believes it helps.
Routes of use and why dose is difficult to measure
| Route | Onset pattern described in article | Measurement problem |
|---|---|---|
| Smoking | Quick, often within minutes | No fixed dose; varies with puff duration, inhalation depth, product concentration, and frequency. |
| Vaping | Quick, often within minutes | No fixed dose; device temperature and cartridge concentration change absorbed amount. |
| Edibles | Slower onset | Longer effects and variable dose relative to label; risk of redosing. |
| Oral oils/capsules | Slower onset | First-pass metabolism changes pharmacology and blood levels over time. |
| Concentrates | Varies by route | A report of 'once a day' may represent a much larger THC exposure than a low-dose edible or a few puffs. |
Route changes exposure. Smoking and vaping deliver cannabinoids to the bloodstream quickly, often within minutes, but they do not deliver a fixed dose. Puff duration, depth of inhalation, product concentration, device temperature, and how frequently the person uses all change the actual absorbed amount. Smoking also exposes the user to carbon monoxide and combustion products. If cannabis is mixed with tobacco, nicotine becomes a major confounder and a direct fetal risk in its own right.
Edibles and oral oils create a different problem. Their onset is slower, their effects last longer, and the dose may be more variable than the label suggests. First-pass metabolism also changes the pharmacology; oral THC produces 11-hydroxy-THC, an active metabolite. That means two products with the same labeled milligrams can feel different and may produce different blood levels over time. Capsules, tinctures, baked goods, beverages, and homemade products all complicate dose estimation.
High-potency concentrates make the measurement problem worse. A patient who reports “once a day” could mean one low-dose edible, one vape session from a 90% THC cartridge, or several inhalations of a concentrate. Those are not equivalent exposures. Yet many observational studies reduce use to yes/no, or to broad frequency categories such as monthly, weekly, or daily. Self-report is common. Biological testing can help, but it has limits too: a urine test may show prior exposure without pinning down timing, route, or exact dose.
This helps explain why the epidemiology is hard to read. SAMHSA reported in 2020 that among pregnant women ages 15 to 44, past-month marijuana use was 3.0% overall, with 5.7% in the first trimester, 3.3% in the second, and 1.8% in the third. Those numbers likely miss some use because people are more likely to deny or minimize stigmatized behavior, especially when disclosure can have legal consequences. So the prevalence data are probably low, while the exposure categories are broad. That is not a good setup for fine-grained risk estimates.
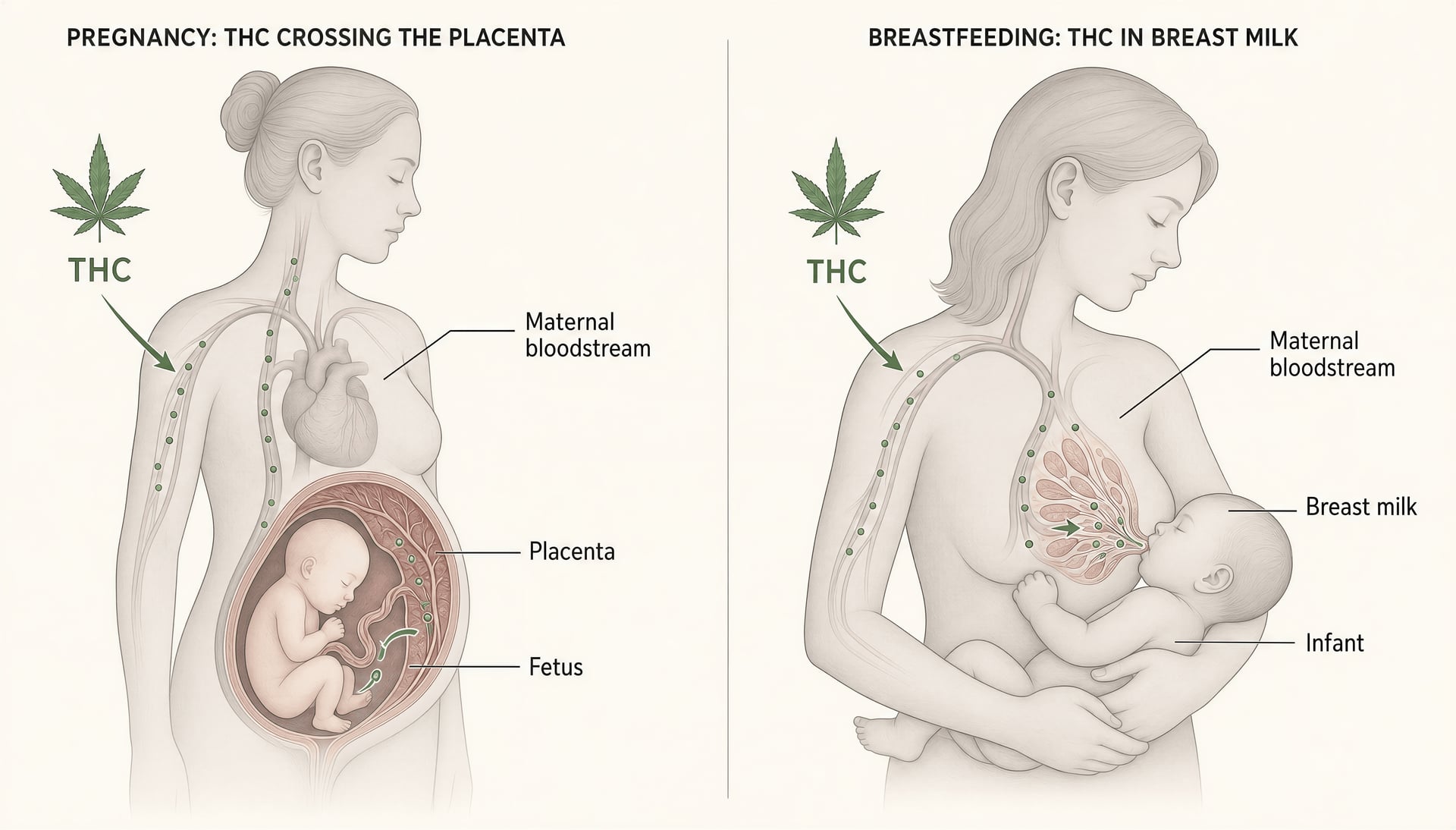
Placental transfer and passage into breast milk
Lipophilic Fat-soluble. A lipophilic drug tends to distribute into fat-rich tissues and fluids, including breast milk, and may persist after obvious intoxication fades.
The pharmacology here is the clearest part of the story. THC is lipophilic, meaning it dissolves readily in fat rather than water. That property matters because the body has many fat-rich tissues, and so does human milk. Lipophilic compounds do not simply appear and vanish on a neat schedule. They distribute into tissues, can be released over time, and may remain detectable beyond the period of obvious intoxication.
THC crosses the placenta. That means fetal exposure is biologically plausible and expected, not speculative. The CDC’s 2024 guidance states that cannabis chemicals pass through the pregnant person’s system to the baby. Once exposure reaches the fetus, concern centers on development, especially because the endocannabinoid system plays a role in brain development. This does not mean every exposure causes harm, and it does not allow a precise prediction for any individual pregnancy. It does mean there is a direct pathway for exposure.
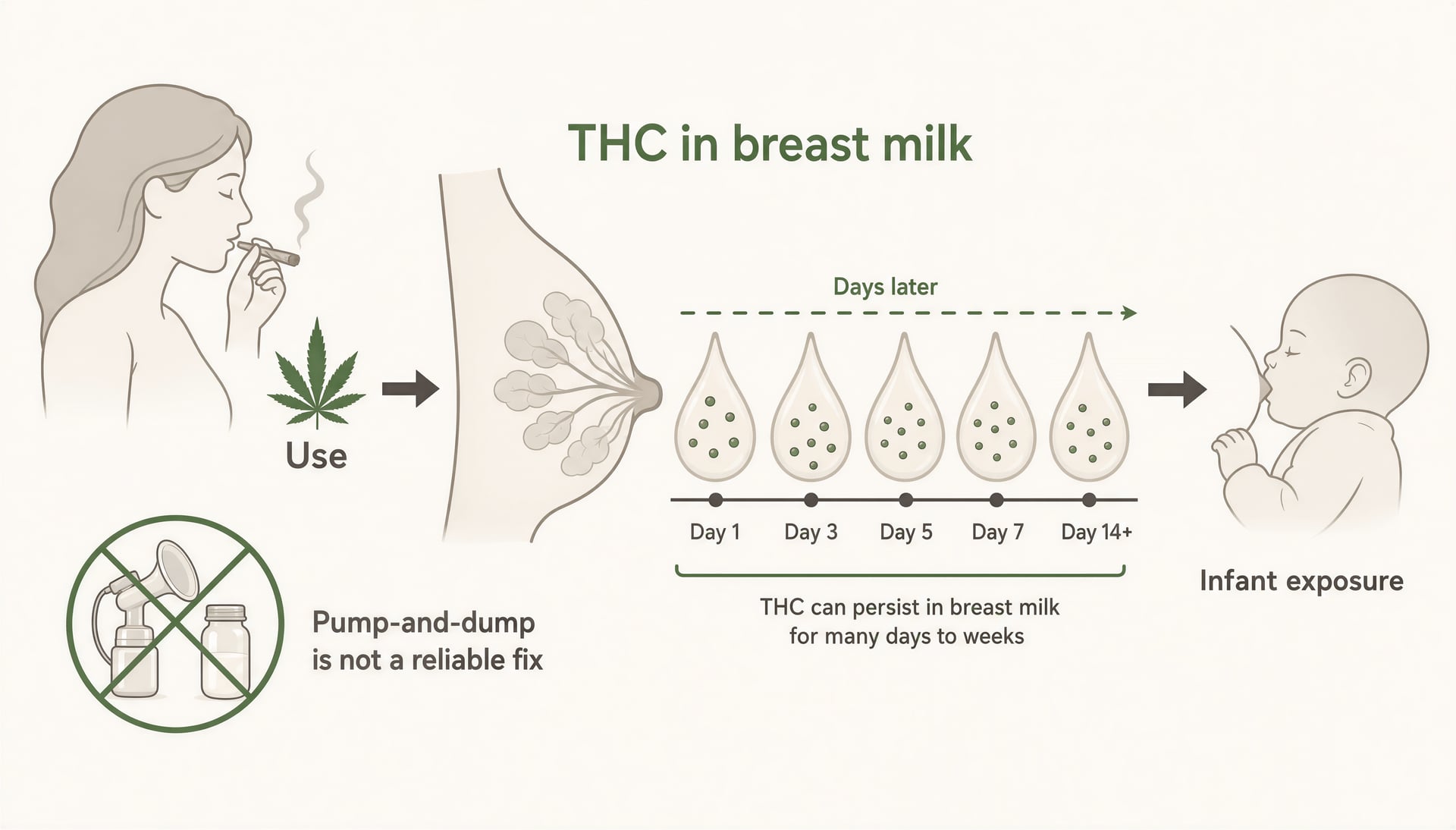
Breast milk raises a related but separate issue. Because milk is fat-rich, THC can accumulate there. The CDC states that breast milk can contain THC for up to 6 days after maternal use, and some studies have found longer durations. That single point undercuts a common myth that timing feeds around use fully prevents infant exposure. “Pump and dump” is not a reliable solution for THC the way it may be discussed for some short-lived substances, because the issue is not just what is in the bloodstream for a few hours. It is storage and slow release.
The evidence on infant outcomes from lactational exposure is thinner than the pregnancy literature. ACOG says data are insufficient to evaluate effects during lactation, and the AAP says the same, which is why both discourage use rather than claim a precisely measured harm. The Academy of Breastfeeding Medicine’s 2023 protocol is slightly more practical in tone, encouraging cessation and reduction while trying to preserve breastfeeding support. That distinction matters. A patient using cannabis should not be frightened away from pediatric care or lactation help. But the exposure itself is real, and the safest interpretation of the current evidence is still avoidance.
How common cannabis use is during pregnancy
[7]National Survey on Drug Use and Health data portal. Substance Abuse and Mental Health Services Administration. SAMHSA Data, 2020. https://www.samhsa.gov/data/
Cannabis use during pregnancy is not rare, and it is not evenly distributed across pregnancy. The clearest national snapshot comes from the Substance Abuse and Mental Health Services Administration. In 2020, SAMHSA estimated that among pregnant women ages 15 to 44, past-month marijuana use was 3.0 percent overall. That average hides a sharp first-trimester peak: 5.7 percent in the first trimester, compared with 3.3 percent in the second and 1.8 percent in the third. Put plainly, measurable use is most common early, often before a pregnancy is recognized or before behavior changes follow a positive test.
That pattern matters because early pregnancy is also when fetal organ development is underway and when many people are dealing with severe nausea, vomiting, appetite disruption, insomnia, and anxiety. It is also the point when someone with frequent pre-pregnancy use may not yet have stopped. So the first-trimester spike is not surprising. It is still concerning.
Chemicals in cannabis, especially THC, pass through the pregnant person's system to the fetus and may harm development.Strong evidence
Clinical advice has been fairly consistent even while the research base remains imperfect. The American College of Obstetricians and Gynecologists stated in Committee Opinion No. 722 in 2017, later reaffirmed in 2021, that “women who are pregnant or contemplating pregnancy should be encouraged to discontinue marijuana use.” The CDC’s 2024 patient guidance is similarly direct: chemicals in cannabis, especially delta-9-tetrahydrocannabinol, or THC, pass through the pregnant person’s system to the fetus and “may harm your baby’s development.” A 2026 report on new guidance made the same point in less academic language: warning against cannabis use during pregnancy remains the standard position. The argument over the evidence is about degree, confounding, and mechanism. It is not about whether major medical groups see prenatal exposure as a risk worth avoiding.
National survey estimates and first-trimester patterns
National surveys almost certainly give a floor, not a ceiling, but they still show a real public-health issue. A 3.0 percent past-month estimate among pregnant women translates into a large absolute number of pregnancies exposed to recent cannabis use each year in the United States. The 5.7 percent first-trimester figure is the number that should reset anyone’s assumptions that prenatal use is vanishingly uncommon.
Other federal summaries from NIH and NIDA have also pointed to rising use over time, especially as cannabis products have become more available and more potent, and as social attitudes have softened outside pregnancy-specific medical settings. But trimester timing is as important as trend lines. A decline from 5.7 percent in the first trimester to 1.8 percent in the third suggests that many people do reduce or stop once pregnancy advances. That is encouraging. It also means early exposure is where much of the burden sits.
Why first-trimester use may be higher
- Some people are using before they know they are pregnant.
- Some continue because symptoms are intense and they believe cannabis helps.
- Some are daily or near-daily users who find stopping difficult.
- Some receive mixed messages from friends, social media, or retail staff who frame cannabis as a natural answer to morning sickness.
The first-trimester pattern likely reflects several overlapping groups. Some people are using before they know they are pregnant. Some continue because symptoms are intense and they believe cannabis helps. Some are daily or near-daily users who find stopping difficult. And some have received mixed messages from friends, social media, or even retail staff who frame cannabis as a natural answer to morning sickness. “Natural” is not a safety category. THC crosses the placenta. That basic pharmacology is not in dispute.

Why self-report likely undercounts use
Self-reported drug use in pregnancy has obvious limits, but cannabis is a special case because the pressure not to disclose can be severe. Stigma plays a role. So does fear. STAT reported in 2026 that, despite expanding legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use. That means a person answering a survey, intake form, or clinic screening question may hear something very different from what the researcher intended. They may hear: could this answer trigger a report, a urine test, a note in my chart, or a CPS referral?
That fear is not irrational. In some health systems, urine toxicology testing is ordered selectively rather than universally, which can pull bias into who gets screened and who gets flagged. Testing may be based on clinician suspicion, prior chart history, insurance status, race, missed visits, or signs of substance use. A positive result can then set legal and child welfare processes in motion, even in places where adult cannabis use is otherwise legal. Punitive systems change behavior. One effect is underreporting. Another is delayed prenatal care, which makes pregnancy outcomes worse for reasons that have nothing to do with THC itself.
There is also a measurement problem. “Past month use” misses people who used earlier in pregnancy and stopped, and it can miss people who understate frequency or type of product. Modern cannabis is not one thing. Exposure varies by route, dose, THC concentration, and co-use with nicotine, alcohol, or other substances. A person who vapes concentrated THC several times a day is not meaningfully captured by the same checkbox as someone who took a few puffs once in the last month. Surveys flatten that difference.
Biological testing can find use that self-report misses, but it is not a clean fix. Urine tests detect metabolites for varying periods depending on frequency of use and body composition, so a positive result does not map neatly onto dose, timing, or impairment. In pregnancy, testing also raises trust and consent concerns. Better surveillance would help research, but not if it drives patients away from care.
Who uses cannabis during pregnancy and why
Pregnant cannabis users are not a single profile, and treating them as one leads to bad care. Some are younger. Some had regular or heavy use before conception and are carrying that pattern into early pregnancy. Some use alongside tobacco or alcohol; others do not. Some have significant stress, depression, trauma history, unstable housing, or limited access to medical care. Some are trying to manage symptoms and believe cannabis is the least harmful option available to them.
Common reasons patients report using cannabis in pregnancy
- Nausea and vomiting
- Poor appetite
- Sleep problems
- Anxiety
- Pain
- Prior dependence or habitual use
The most commonly reported reasons are practical and immediate: nausea, vomiting, poor appetite, sleep problems, anxiety, pain, and prior dependence or habitual use. Morning sickness is a recurring theme, especially in the first trimester, which helps explain why prevalence is highest then. But a common reason is not the same thing as a good reason medically. ACOG specifically advises that pregnant patients should be encouraged to discontinue cannabis, including when it is being used for medicinal purposes, in favor of treatments with better pregnancy safety data.
That distinction matters because a patient using cannabis for symptom relief is often making a tradeoff under pressure, not making a statement about safety. If prescribed antiemetics have failed, if insomnia is relentless, or if stopping a long-standing daily habit produces withdrawal-like irritability and sleep disruption, “just stop” is not much of a clinical plan. Non-punitive counseling is. So is offering alternatives that actually address the symptom driving use.
The social map of use also overlaps with inequality. Criminalization and surveillance do not fall evenly. The same behavior can lead to very different consequences depending on where someone lives, what hospital they attend, and how they are perceived. That is one reason prevalence data should never be read as simple behavior counts. They are filtered through disclosure risk.
So how common is cannabis use during pregnancy? Common enough that every prenatal care system should expect to encounter it routinely, especially in the first trimester. Common enough that self-report figures are almost surely low. And common enough that public health messaging needs to do two things at once: state clearly that major medical bodies advise avoiding cannabis in pregnancy, and make it safer for patients to tell the truth about use without fearing punishment.
Why some pregnant patients use cannabis despite medical advice
The first thing many public discussions miss is simple: people do not usually use cannabis in pregnancy because they are careless. They use it because they are trying to manage something hard—vomiting that will not stop, panic that spikes at night, pain that makes sleep impossible, appetite loss, trauma symptoms, or a long-standing pattern of use that predates pregnancy and is not easy to stop on command. That does not make cannabis a recommended treatment in pregnancy. It does explain why “just don’t” often fails as a clinical response.
Mainstream medical guidance is clear. ACOG’s Committee Opinion No. 722, issued in 2017 and reaffirmed in 2021, says pregnant people “should be encouraged to discontinue marijuana use.” The CDC states in 2024 that THC and other chemicals in cannabis pass to the fetus and “may harm your baby’s development.” In 2026, new guidance again warned against cannabis use during pregnancy because potential fetal risks are not offset by proven safety. The problem is not a lack of warnings. The problem is that symptom burden and treatment access often do not match those warnings.
That gap matters. It also helps explain why use appears highest early in pregnancy, when nausea, vomiting, and uncertainty are often worst. SAMHSA reported in 2020 that past-month marijuana use among pregnant women ages 15 to 44 was 3.0 percent overall, but 5.7 percent in the first trimester, compared with 3.3 percent in the second and 1.8 percent in the third. Self-report likely misses some use. Even so, the pattern fits what clinicians hear every day: the first trimester is where many patients are most desperate for relief.
Nausea and hyperemesis claims
Pregnancy nausea is common. Hyperemesis gravidarum is something else entirely: severe, sometimes dangerous vomiting that can lead to dehydration, weight loss, electrolyte problems, and repeated ER visits. A patient who says cannabis is the only thing that lets her keep food down is not making a trivial claim.
Some do report exactly that. Prior cannabis use before pregnancy can shape expectations, and social networks often reinforce the idea that inhaled or edible cannabis works faster or feels more effective than prescribed anti-nausea drugs. But professional bodies still advise against it. The reason is straightforward. Evidence for symptom relief in pregnancy is largely anecdotal, while fetal safety evidence is not reassuring enough to treat cannabis as an acceptable antiemetic.
That distinction gets lost online. Cannabis has recognized anti-nausea effects in some non-pregnant settings, especially with chemotherapy-related nausea, but that does not answer the pregnancy question. Pregnancy is different because the treatment reaches a fetus during a period of rapid neurodevelopment. Delta-9-tetrahydrocannabinol is lipophilic and crosses the placenta. So even if a patient feels better, the safety tradeoff remains unresolved.
The research base also has a selection problem. Patients with severe nausea may be more likely to use cannabis, which makes it hard to separate the effects of the drug from the effects of the underlying illness. Some reports have even raised the possibility that cannabis can complicate the clinical picture in heavy users, including overlap with cannabinoid hyperemesis syndrome. That does not mean every pregnant patient using cannabis for nausea has that syndrome. It does mean “it helps nausea” is not always the whole story.
Clinicians should take the symptom seriously and the treatment claim skeptically. If a patient is using cannabis because she has vomited for days and cannot function, the answer is not moral scolding. It is urgent symptom treatment, hydration when needed, medication review, and follow-up. Still, the medical recommendation remains avoidance, because evidence of benefit is not matched by evidence of fetal safety.
Mental health, insomnia, and pain
Not all cannabis use in pregnancy is about nausea. A large share is about distress. Patients may be trying to dampen anxiety, sleep through insomnia, blunt PTSD symptoms, reduce back pain, improve appetite, or cut down on other substances they see as worse. That logic can feel practical from the patient side, especially if prior use seemed helpful or if prescribed alternatives caused side effects.
Pregnancy can also disrupt existing psychiatric treatment. Some patients stop medications abruptly after seeing alarming posts online. Others lose access to therapy, cannot find a prescriber comfortable treating them in pregnancy, or fear judgment if they admit relapse, panic, or depression. Cannabis then becomes a familiar fallback.
Medical guidance still does not endorse it for those uses. The issue is not only potential fetal risk. It is also that cannabis is an inconsistent product category. THC concentration has risen over time. Products vary widely by dose, route, timing of absorption, and co-occurring cannabinoids. What a patient means by “a little cannabis to sleep” could range from occasional low-dose inhalation to high-potency concentrates or repeated edible use with prolonged exposure. Research from earlier eras, when average potency was lower, does not map neatly onto the current market.
At the same time, the outcome data remain hard to interpret. Reviews have found associations between prenatal cannabis exposure and lower birth weight, and some studies suggest higher odds of preterm birth or NICU admission. There are also signals in later attention, executive function, or behavior. But many studies are tangled with tobacco exposure, alcohol use, poverty, stress, racism, limited prenatal care, and reliance on self-report. That is why careful reporting says mixed evidence, not no evidence. Mixed does not mean harmless.
For clinicians, the right move is not to pretend certainty where none exists, but to be clear about the direction of guidance. For anxiety, insomnia, and pain in pregnancy, cannabis is discouraged because potential benefit is uncertain and fetal safety is not established. Patients need substitutes, not slogans.

The influence of social media and dispensary-era normalization
The legal market changed the social meaning of cannabis faster than the evidence changed. In many places it now looks ordinary: sold in regulated storefronts, recommended in casual conversation, packaged like wellness products, and discussed online as if “natural” were the same as safe in pregnancy. It is not.
Social media accelerates this. A pregnant person searching “morning sickness relief” may find hundreds of personal testimonials before she finds ACOG or CDC guidance. Short videos and forum posts often frame cannabis as gentler than prescription medication, safer than alcohol, or unfairly stigmatized by older medicine. Some dispensary workers have reportedly suggested products for nausea or sleep despite the lack of pregnancy safety evidence. That advice can feel credible because it is confident, immediate, and tailored to symptoms.
Normalization also interacts with distrust. Patients who have felt dismissed by the health system may put more weight on peer stories than on official warnings, especially when those warnings arrive without symptom relief. Yet legalization has not removed the risk of punishment. STAT reported in 2026 that pregnant people can still face child welfare investigations and criminal penalties for cannabis use despite expanding legalization. That contradiction matters. Society tells patients cannabis is ordinary, then treats them as neglectful if they disclose use in pregnancy.
The result is a bad policy-clinic mix: normalization in the marketplace, uncertainty in the evidence, and punishment in the background. That can drive use underground and make honest prenatal counseling less likely. Non-punitive care is the better approach. Patients need accurate information, practical alternatives for nausea, insomnia, pain, and mental health symptoms, and a care setting where disclosure does not feel like a trap. That is how medical advice becomes usable, rather than just official.
What major medical organizations currently recommend
| Organization | Year cited | Pregnancy guidance | Breastfeeding guidance |
|---|---|---|---|
| ACOG | 2017; reaffirmed 2021 | Pregnant or contemplating-pregnancy patients should be encouraged to discontinue marijuana use. | Insufficient data to evaluate infant effects; in the absence of such data, marijuana use is discouraged. |
| CDC | 2024 | Do not use cannabis in pregnancy; THC and other chemicals pass to the baby and may harm development. | Breast milk can contain THC for up to 6 days after use; breastfeeding use is discouraged. |
| AAP | 2018 | Discourages use during pregnancy. | Data are insufficient to assess infant effects; maternal marijuana use while breastfeeding is discouraged. |
| Academy of Breastfeeding Medicine | 2023 | Not the primary pregnancy guidance body in the article. | Encourages cessation and/or reduction of cannabis use during breastfeeding. |
The striking part of current guidance is how consistent it is on the practical bottom line, even though the evidence base is incomplete in places. Major U.S. medical and public-health bodies do not tell pregnant patients that every reported association is proven causation. They do not claim the lactation data are settled. But they still land in the same place: avoid cannabis during pregnancy, stop if you are trying to conceive or become pregnant, and do not use cannabis while breastfeeding if you can avoid it. Just as important, they generally call for counseling and support rather than punishment.
That last point matters because policy and practice do not always line up. STAT reported in 2026 that “despite expanding cannabis legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use,” even while “the evidence on cannabis use in pregnancy remains mixed.” Clinical guidance is written against that backdrop. A punitive response can push people away from prenatal care. Medical organizations have increasingly tried to frame screening as a route to treatment and safer care, not a trap door into criminalization.
ACOG and obstetric guidance
The American College of Obstetricians and Gynecologists has been clear for years. In Committee Opinion No. 722, first issued in 2017 and reaffirmed in 2021, ACOG states: “Women who are pregnant or contemplating pregnancy should be encouraged to discontinue marijuana use.” That is the core recommendation. Not cut down if convenient. Discontinue.
ACOG also tells obstetric clinicians to ask about use early. The opinion says that “before pregnancy and in early pregnancy, all women should be asked about their use of tobacco, alcohol, and other drugs, including marijuana.” This is a standard-of-care screening message, but ACOG pairs it with a second instruction that often gets lost in public debate: counseling should be aimed at treatment and support, and patients should be informed about possible mandatory reporting consequences. ACOG explicitly warns against turning screening into punishment. The committee opinion says patients should be told that the purpose of screening is to allow treatment, “not to punish or prosecute her,” though it also acknowledges that state laws may still impose reporting duties.
That distinction is not a side issue. It is central. If pregnant patients believe disclosure will trigger child welfare involvement, they may avoid prenatal care or withhold information about substance use, nausea self-treatment, or other exposures. ACOG has long opposed criminal and civil penalties that deter care during pregnancy.
On the science, ACOG takes a cautious but not exaggerated line. It notes concerns about impaired neurodevelopment and fetal exposure to smoke, and it points out that delta-9-tetrahydrocannabinol, or THC, crosses the placenta. The organization does not present every adverse outcome as conclusively caused by cannabis alone. It recognizes that many studies are limited by confounding from tobacco, alcohol, other drug use, nutrition, stress, and socioeconomic factors. Potency has also changed sharply over time, which makes older studies harder to map onto current products. Still, ACOG sees enough concern to recommend abstinence during pregnancy.
That applies to medical use too. ACOG advises that pregnant people or those considering pregnancy should discontinue cannabis even when they are using it for medicinal reasons and should switch to an alternative therapy with better pregnancy-specific safety data. This is especially relevant because some patients use cannabis for nausea and vomiting in early pregnancy, the same period when use peaks. SAMHSA reported in 2020 that among pregnant women ages 15 to 44, past-month marijuana use was 3.0 percent overall, but 5.7 percent in the first trimester, compared with 3.3 percent in the second and 1.8 percent in the third. A first-trimester pattern like that fits with self-medication for nausea, but ACOG does not endorse cannabis as an antiemetic in pregnancy.
Lactation gets its own carefully worded statement from ACOG: “There are insufficient data to evaluate the effects of marijuana use on infants during lactation and breastfeeding, and in the absence of such data, marijuana use is discouraged.” That wording matters because it shows how these recommendations are built. ACOG is not saying the evidence is perfect. It is saying uncertainty is not a reason for reassurance when infant exposure is plausible and avoidable.
CDC and public-health messaging
The Centers for Disease Control and Prevention uses more direct public-facing language. Its 2024 pregnancy page states: “The chemicals in cannabis (in particular, tetrahydrocannabinol or THC) pass through your system to your baby and may harm your baby’s development.” CDC tells people who are pregnant or planning pregnancy not to use cannabis in any form. That includes smoking, vaping, dabbing, eating edibles, and using topical or concentrated products where systemic absorption can still occur.
CDC messaging is less tied to the technical language of committee opinions and more focused on risk communication. The agency emphasizes that THC is lipophilic, crosses the placenta, and reaches the developing fetus. It also warns that cannabis smoke contains many of the same toxins as tobacco smoke, which matters because smoked cannabis is still a common route of exposure. Public-health language often has to be simple, and CDC does simplify. But the agency is not inventing a certainty that specialists reject. It is making a preventive recommendation under uncertainty, which is standard public health when fetal or infant exposure may carry developmental risk.
The CDC also points to possible harms that have shown up repeatedly in observational research: lower birth weight and abnormal neurologic development among them. Those findings are not equally strong across every study, and residual confounding remains a major problem. Even so, the signal has been concerning enough that no mainstream U.S. health authority recommends cannabis use in pregnancy.
A 2026 trade-press report described “new guidance warns against cannabis use during pregnancy because of potential fetal risks.” That did not mark a reversal. It reflected continuity. As products have become more potent and legalization has expanded, the guidance from medical and public-health bodies has stayed remarkably stable: don’t use cannabis during pregnancy, and if a patient is using it, respond with counseling, education, and help stopping.
AAP and Academy of Breastfeeding Medicine on lactation
Breastfeeding guidance is where the wording becomes especially careful, because the evidence base is thinner than in pregnancy. The American Academy of Pediatrics, in its 2018 clinical report on marijuana use during pregnancy and breastfeeding, states: “Data are insufficient to assess the effects of exposure of infants to maternal marijuana use during breastfeeding. As a result, maternal marijuana use while breastfeeding is discouraged.” Again, the structure is important. Insufficient data does not become a green light.
The CDC echoes that line and adds a concrete pharmacology point that clinicians often cite: “Breast milk can contain THC for up to 6 days after use, according to one study. Other studies have noted even longer duration.” Because THC is stored in body fat and released over time, pumping and discarding milk right after use is not a reliable workaround. Exposure may persist.
The Academy of Breastfeeding Medicine took up this issue in Clinical Protocol #21, revised in 2023. Its wording is direct but not absolutist: “We encourage cessation and/or reduction of cannabis use during breastfeeding.” ABM’s protocol is notable because it tries to balance the known benefits of breastfeeding with concern about drug transfer into milk and the reality that some parents will not be able or willing to stop immediately. That produces a slightly different tone from a simple prohibition. ABM does not endorse cannabis use during lactation. It recommends helping mothers stop or reduce use, assessing for substance use disorder, and providing individualized care rather than reflexively cutting off breastfeeding support.
That is a meaningful distinction. “Discouraged” and “encourage cessation and/or reduction” are not identical phrases, but they point in the same direction. Avoid infant THC exposure. Do not present cannabis as harmless during lactation. Do not overclaim certainty where the data are weak. And do not punish people out of care.
Put plainly, the major organizations agree on the practical advice. ACOG says pregnant or contemplating-pregnancy patients should discontinue. CDC says the chemicals in cannabis pass to the baby and may harm development. AAP says breastfeeding use is discouraged because the infant-effect data are insufficient. ABM says to encourage cessation or reduction during breastfeeding. The wording changes by audience, but the message does not.
What the evidence says about pregnancy outcomes
The central fact is simple: major medical groups advise avoiding cannabis during pregnancy, yet the research behind specific pregnancy outcomes is uneven. ACOG’s Committee Opinion No. 722, first issued in 2017 and reaffirmed in 2021, says pregnant patients or those contemplating pregnancy “should be encouraged to discontinue marijuana use.” The CDC in 2024 stated that chemicals in cannabis, especially delta-9-tetrahydrocannabinol (THC), pass to the fetus and may harm development. That guidance is not built on a single dramatic finding. It comes from a pattern of concern across studies, with some signals showing up more consistently than others.
That distinction matters because public discussion often swings between two bad extremes. One says cannabis exposure is obviously catastrophic and proven to cause every bad outcome. The other shrugs that the data are too messy to say anything at all. Neither is accurate. THC is lipophilic, crosses the placenta, and reaches the developing fetus. Prenatal exposure is biologically plausible as a risk. But in population studies, cannabis use during pregnancy is entangled with tobacco, alcohol, other drugs, untreated nausea, poverty, stress, intimate partner violence, housing instability, and barriers to prenatal care. STAT reported in 2026 that even as legalization spread, pregnant people still faced child welfare investigations and criminal penalties for cannabis use, and that the evidence base remained mixed. That legal reality can itself distort the data by making honest disclosure less likely and delaying care.
Use during pregnancy is not rare, especially early on. SAMHSA reported in 2020 that among pregnant women ages 15 to 44, past-month marijuana use was 3.0 percent overall, including 5.7 percent in the first trimester, 3.3 percent in the second, and 1.8 percent in the third. Those figures probably undercount actual exposure because self-report in a punitive environment is unreliable. The first trimester peak also suggests that some use happens before pregnancy recognition, while some is tied to nausea and vomiting.
Miscarriage, fetal growth, and birth weight
The evidence linking prenatal cannabis exposure to miscarriage is concerning but inconsistent.Limited evidence
Miscarriage is one of the hardest outcomes to study well. Early pregnancy loss is common, many losses occur before a person knows they are pregnant, and exposure measurement is often poor. Some studies have reported higher odds of miscarriage among cannabis users, while others have not found a clear independent association after adjustment. At this point, the evidence for miscarriage is concerning but inconsistent. It is not the strongest part of the case against prenatal cannabis exposure.
Lower birth weight is one of the more consistent outcome signals in the prenatal cannabis literature.Strong evidence
Fetal growth and birth weight are different. Here, the signal is more persistent.[8]Prenatal exposure to cannabis and maternal and child health outcomes: a systematic review and meta-analysis. J.K.L. Gunn, A.B. Rosales, K.M. Center, et al.. BMJ Open, 2016. https://bmjopen.bmj.com/content/6/4/e009986
A 2016 meta-analysis by Gunn and colleagues in BMJ Open examined prenatal cannabis exposure and adverse maternal and neonatal outcomes. One of its clearest findings was an association with lower birth weight, although many included studies had major confounding issues. That same year, ACOG cited the lower-birth-weight pattern as one of the more repeatable findings in the literature. Later reviews have largely landed in the same place: if there is one obstetric outcome that appears again and again, it is reduced fetal growth or a modest shift toward lower birth weight.
This does not mean every exposed infant is small for gestational age, or that cannabis alone explains the result in any individual pregnancy. It means that across groups, exposed pregnancies tend to show a weight penalty more often than not. Some studies detect higher rates of birth weight under 2,500 grams. Others find lower mean birth weight without a large jump in the strict low-birth-weight category. Still others report smaller head circumference or shorter birth length, though those findings are less stable.
One reason the birth-weight signal deserves attention is biological plausibility. Placental function is sensitive to vascular, inflammatory, and endocrine changes. Cannabinoid receptors are present in reproductive tissues and the placenta, which gives researchers a mechanism worth taking seriously even before the epidemiology is perfect. Another reason is consistency: even when studies disagree on magnitude, many point in the same direction.
Yet caution is still needed. Older studies often reflect lower-THC products than what is common now. Some classified “marijuana use” as any use during pregnancy, without dose, route, or timing. Others relied entirely on self-report, which misses intermittent or stigmatized use. A patient using a high-potency concentrate daily is not meaningfully equivalent to someone who used cannabis twice before learning they were pregnant, but many datasets collapse both into the same exposure group. That weakens precision.
The best reading of the evidence is this: lower birth weight and fetal growth restriction are not proven to be caused solely by cannabis in every case, but the association is repeated often enough that clinicians are justified in treating it as a real risk signal rather than background noise.
Preterm birth, stillbirth, and NICU admission
| Outcome | How the article characterizes the evidence |
|---|---|
| Lower birth weight / fetal growth restriction | More repeated and comparatively consistent signal across reviews and cohorts. |
| Preterm birth | Frequently reported and biologically plausible, but less consistent after adjustment for tobacco and other confounders. |
| Stillbirth | Raises concern in some studies, but hard to separate from smoking and other confounding factors. |
| NICU admission | Often higher in exposed groups, but may reflect downstream effects such as lower birth weight or prematurity and local practice patterns. |
| Major congenital anomalies | No specific consistent pattern established the way it has been for some other teratogens. |
Preterm birth is more contested. Some cohort studies and reviews have found increased odds of delivery before 37 weeks among cannabis-exposed pregnancies. Others have found the association fades after controlling for tobacco or other substances. The 2016 Gunn meta-analysis reported increased odds of preterm delivery in some comparisons, but the effect was not uniformly stable across adjusted analyses. Since then, larger observational studies have continued to report concern, but the story remains less settled than it is for birth weight.
A fair way to put it is that preterm birth is possible, plausible, and frequently reported, but not pinned down with the same consistency. The direction of effect often points toward elevated risk. The confidence that cannabis is independently responsible is lower.[9]Association Between Stillbirth and Illicit Drug Use and Smoking During Pregnancy. M.W. Varner, R.M. Silver, D.J. Hogue, et al.. Obstetrics & Gynecology, 2014. https://pubmed.ncbi.nlm.nih.gov/24553166/
Stillbirth is even harder to parse. One often-cited source is the Stillbirth Collaborative Research Network study published by Varner and colleagues in 2014, which found tetrahydrocannabinolic acid in umbilical cord homogenate was associated with stillbirth. But the authors and later commentators were careful: cigarette smoking and other confounding factors could not be fully separated. That caution matters because stillbirth is strongly linked to a wide range of social and medical risks that cluster with substance use. So the existing literature raises concern, but it does not support simple claims that cannabis exposure has been cleanly shown to cause stillbirth on its own.
NICU admission sits somewhere between birth weight and preterm birth in terms of consistency. Several studies and reviews have found higher NICU admission rates among infants with prenatal cannabis exposure. On paper, that can sound more definitive than it is. NICU admission is not a disease. It is an outcome shaped by hospital policy, monitoring intensity, gestational age, feeding issues, low birth weight, and local practice patterns. If exposed infants are more likely to be small or born a bit early, NICU admission may rise as a downstream marker rather than a direct toxic effect. Even so, it is clinically meaningful. Families care about whether a newborn needs intensive care, regardless of the causal pathway.
The same caution applies to Apgar scores and congenital anomalies. Findings are mixed, and no specific pattern of major structural malformations has been consistently established for prenatal cannabis exposure the way it has for some other teratogens. That does not make exposure safe. It means the strongest obstetric concerns are not major birth defects but growth, possibly prematurity, and related neonatal complications.
What happens when tobacco and other substances are accounted for
This is where interpretation gets difficult and where a lot of bad reporting goes wrong.
Cannabis use in pregnancy often overlaps with cigarette smoking, nicotine vaping, alcohol use, and use of other drugs. Tobacco is the biggest confounder in many studies because it is strongly tied to low birth weight, placental problems, and preterm birth. If a study reports that cannabis exposure predicts a 150-gram drop in birth weight but most of the exposed group also smokes cigarettes, the key question is what remains after careful adjustment.
Sometimes the association shrinks. Sometimes it disappears. Sometimes it persists.
That pattern does not mean the cannabis effect is fake. It means the estimate is unstable because real life exposures cluster together. Statistical adjustment can help, but it cannot fully solve bad measurement. “Tobacco use” may mean anything from one cigarette a week to a pack a day. “Cannabis use” may mean a single edible, daily smoking, or concentrated products with far higher THC content than older datasets captured. Residual confounding is almost unavoidable.
Stress and access to care matter too. Patients who use cannabis during pregnancy are, on average, more likely in many cohorts to face socioeconomic strain, food insecurity, unstable housing, racism in health care, or fear of punitive reporting. Those conditions affect pregnancy outcomes on their own. They also affect whether someone gets early prenatal care, treatment for nausea, blood-pressure monitoring, infection screening, or support for quitting cigarettes. A model that adjusts for income and education alone does not erase those differences.
There is also confounding by indication. Some pregnant patients use cannabis because they have severe nausea, anxiety, chronic pain, or insomnia. Hyperemesis itself can affect weight gain and pregnancy course. If researchers do not separate the effect of the symptom from the effect of the drug used to manage it, the picture blurs further.
Even with all that, the safest evidence-based position is not agnosticism. It is caution. The mixed literature does not clear cannabis. It shows repeated association signals, especially for fetal growth and lower birth weight, alongside less consistent but still concerning signals for preterm birth and NICU admission. Professional guidance reflects exactly that balance. The advice to avoid cannabis during pregnancy is stronger than the proof for any single outcome because the potential fetal risk is credible, the upside is limited, and cleaner alternatives exist for many symptoms.
What the evidence says about neurodevelopment
The hardest question in this area is not whether THC reaches the fetus. It does. Delta-9-tetrahydrocannabinol is lipophilic, crosses the placenta, and later appears in breast milk; CDC stated in 2024 that breast milk can contain THC for up to 6 days after maternal use, with some studies finding longer persistence. The harder question is what that exposure does to neurodevelopment, and how confidently researchers can separate cannabis from everything that often travels with it: tobacco, alcohol, poverty, stress, maternal mental illness, unstable housing, and differences in the postnatal home environment.
That distinction matters because public discussion often jumps from “exposure exists” to “long-term brain damage is proven.” The science is not that clean. But neither is it reassuring enough to dismiss. Major medical bodies take a clear position anyway. ACOG’s Committee Opinion No. 722 said in 2017, reaffirmed in 2021, that pregnant patients should be encouraged to discontinue marijuana use. The American Academy of Pediatrics and the Academy of Breastfeeding Medicine also discourage use during pregnancy and lactation. They are responding to a literature base that shows repeated signals of risk, especially in attention, behavior, and executive function, even though effect sizes are often modest and causal certainty remains incomplete.
Infant and early childhood findings
Studies that focus on infancy and the preschool years do not show a single, uniform pattern. Some report little difference on broad developmental screens. Others find small but concerning shifts in domains tied to self-regulation, language, attention, or problem-solving.
Part of the reason is measurement. A crude global screen at 12 months may miss subtle effects that become more visible when tasks demand impulse control or sustained attention at age 4, 7, or 10. Another problem is that older cohorts were often studying lower-potency cannabis than what is common now, so “no large effect” in a cohort recruited in the 1980s does not necessarily settle the question for high-THC products used in the 2020s.
Two long-running prospective cohorts are cited constantly here: the Ottawa Prenatal Prospective Study, begun in 1978, and the Maternal Health Practices and Child Development Study in Pittsburgh, begun in 1982. Those studies found mixed early results but recurring signals later in childhood. In infancy, findings were often weak or inconsistent on general cognitive scores. That inconsistency has sometimes been misread as evidence of safety. It is not. It may simply mean early developmental tests were blunt instruments for detecting later-emerging problems in attention control and higher-order cognition.
More recent work, including analyses of large administrative and health-system datasets, has also been mixed. Some studies have reported associations between prenatal cannabis exposure and developmental delay or communication concerns in early childhood; others have found attenuation after adjustment for confounders. A 2024 Kaiser Permanente Northern California cohort by Young-Wolff and colleagues, for example, examined maternal prenatal cannabis use and child developmental outcomes and found that associations could shift meaningfully depending on outcome definitions and adjustment strategy. That is typical in this field. A signal appears, then shrinks when tobacco exposure, maternal education, psychiatric history, or neighborhood deprivation is added to the model.
Still, the pattern is not random noise. Systematic reviews and meta-analyses over the past decade have repeatedly landed in the same general place: prenatal cannabis exposure is associated with small increases in the risk of adverse neurodevelopmental or behavioral outcomes, but confidence in any single effect estimate is limited by study quality and confounding. “Association” is the right word. Not proof. Not exoneration.
The same caution applies to breastfeeding-only exposure, where the evidence is thinner. Because THC is excreted into milk and persists there, concern is biologically plausible. Yet lactation studies are sparse, often small, and badly confounded by prenatal exposure. If an infant exposed through breast milk was also exposed in utero, and grows up in a household shaped by the same social and medical stresses linked to substance use, it becomes very hard to isolate the independent contribution of milk-borne THC.
Attention, executive function, and behavior over time
Executive function A set of higher-order mental processes used to plan, focus attention, control impulses, hold information in mind, and regulate behavior.
Where the literature becomes more concerning is not infant IQ but later function. Attention. Inhibition. Working memory. Behavioral regulation.
Neurodevelopmental domains discussed most often
- Sustained attention
- Impulse control
- Planning
- Visual problem-solving
- Short-term memory
- Behavioral regulation
Several cohort studies have reported that children and adolescents with prenatal cannabis exposure score worse, on average, on tasks involving sustained attention, impulse control, planning, visual problem-solving, or short-term memory. The effect sizes are usually not huge. We are not talking about every exposed child having a major disability. We are talking about shifts in group averages and a possible increase in the odds of clinically meaningful problems for some children.[10]Prenatal marijuana and alcohol exposure and academic achievement at age 10. L. Goldschmidt, N.L. Day, G.A. Richardson. Neurotoxicology and Teratology, 2008. https://pubmed.ncbi.nlm.nih.gov/19004561/
The Ottawa cohort reported associations over time between prenatal cannabis exposure and deficits in higher-order cognitive functions, including aspects of executive functioning and attention, especially as children reached school age and adolescence. The Pittsburgh Maternal Health Practices and Child Development Study similarly linked heavier prenatal exposure with problems in impulsivity, hyperactivity, attention, and delinquency-related behaviors later on. Goldschmidt and colleagues, in a 2008 paper from the Pittsburgh cohort, found that prenatal marijuana exposure predicted problems in attention and delinquency in 10-year-olds even after adjustment for several confounders. That result gets cited often because it moved beyond broad intelligence measures and focused on the kinds of functions teachers and parents notice in daily life.[11]Associations Between Prenatal Cannabis Exposure and Childhood Outcomes: Results From the ABCD Study. S.E. Paul, R. Hatoum, A.R. Fine, et al.. JAMA Psychiatry, 2020. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2765199
More recent population-based studies have not erased those concerns. Some have found associations between prenatal cannabis exposure and increased rates of attention problems, externalizing behavior, or symptoms relevant to ADHD. Others found no statistically clear link after fuller adjustment. A 2020 study using the Adolescent Brain Cognitive Development cohort by Paul and colleagues reported that cannabis exposure after maternal knowledge of pregnancy was associated with more child psychopathology, attention problems, and social issues. Critics quickly pointed out that observational adjustment can only go so far, and that unmeasured confounding remained likely. They were right to say so. But it is also true that the study fit a longer-running pattern rather than standing alone.
A large across-the-board drop in general intelligence from prenatal cannabis exposure is not well supported by current evidence.Limited evidence
What does not seem well supported is a sweeping claim that prenatal cannabis exposure causes a large drop in general intelligence across the board. The evidence there is weaker and less consistent. Many studies find little or no stable difference in overall IQ once confounders are handled. The signals are more specific than that. They cluster around regulation, behavior, and executive control.
That specificity makes biological sense. The fetal endocannabinoid system is involved in neurodevelopmental processes, including neuronal migration and synapse formation. Interfering with that signaling during sensitive periods could plausibly affect circuits involved in attention and self-regulation more than broad global intelligence. Plausible, however, is not the same as definitively shown in humans.
A defensible bottom line is this: there is enough evidence of potential harm in attention, behavior, and executive function to justify clear clinical advice to avoid cannabis during pregnancy, but not enough precision to claim a fixed dose-response rule or to predict outcomes for any individual child.
Why long-term developmental studies are so difficult
This literature is messy because real life is messy.
Start with residual confounding. Pregnant cannabis users are, on average, more likely in many datasets to also use nicotine, alcohol, or other substances, and more likely to experience stressors that independently shape child development. Even when researchers statistically adjust for these factors, adjustment is only as good as the data. Self-report undercounts use. Timing is often vague. Frequency categories like “weekly” or “monthly” tell you very little about dose.
Then there is product change over time. Much of the classic literature tracks pregnancies from the late 1970s through the 1990s, when average THC potency was far lower than current commercial products. Concentrates, high-THC flower, and repeated daily use were not represented in the same way. A child exposed to a product averaging 3 to 5 percent THC is not necessarily comparable to one exposed to products that can exceed 20 percent THC, let alone extracts.
Home environment matters too, and not as a nuisance variable but as part of the causal web. A child’s language exposure, sleep stability, nutrition, school quality, caregiver mental health, and exposure to adversity can either buffer or magnify developmental vulnerabilities. Some cohorts try to measure this. None measure it perfectly.
Attrition is another chronic problem. Longitudinal studies lose participants, and loss is rarely random. Families under the greatest strain are often the hardest to follow for 10 or 15 years, which can bias results in either direction. By adolescence, the sample that remains may no longer represent the original cohort well.
Finally, postnatal exposure complicates the picture. If a child was exposed prenatally, then again through breast milk, then through secondhand cannabis smoke or household dysfunction, what exactly is being estimated? Very often, the answer is not “the isolated effect of prenatal THC” but “the developmental pattern seen among children born into a cluster of exposures.”
That is why the evidence remains mixed, as STAT reported in 2026, even while clinical guidance remains firm. Mixed does not mean neutral. It means the data show enough concerning signals that professional societies advise avoidance, while researchers continue arguing over magnitude, mechanism, and causality. For neurodevelopment, the most honest reading is neither panic nor shrugging reassurance. It is concern with uncertainty attached.
Breastfeeding and cannabis: what is known, what is not
- Established fact
- THC enters breast milk
- Persistence
- CDC says up to 6 days after use; some studies report longer
- Infant-outcome evidence
- Limited and hard to isolate from prenatal exposure
- ACOG
- Use is discouraged because data are insufficient
- AAP
- Maternal marijuana use while breastfeeding is discouraged
- ABM
- Encourage cessation and/or reduction
Breastfeeding is where public messaging often becomes least careful. Some warnings imply that any cannabis exposure through milk is so dangerous that nursing should automatically stop. Other messages shrug and suggest that because the research is thin, there is probably little to worry about. Neither position matches the evidence. What is clearly established is pharmacology: delta-9-tetrahydrocannabinol, or THC, enters breast milk. What remains unsettled is the size of the infant dose across different patterns of use, and how much that exposure changes infant health or development in the short or long term.
That gap matters because clinicians are weighing two real things at once: the known value of human milk and breastfeeding support, and the plausible but still incompletely measured risks of cannabinoid exposure during a period of rapid brain development. Major medical groups do not treat that uncertainty as reassurance. ACOG stated in Committee Opinion No. 722, first issued in 2017 and reaffirmed in 2021, that there are “insufficient data to evaluate the effects of marijuana use on infants during lactation and breastfeeding, and in the absence of such data, marijuana use is discouraged.” The American Academy of Pediatrics said much the same in 2018. The Academy of Breastfeeding Medicine, in Clinical Protocol #21 revised in 2023, moved toward a practical harm-reduction frame: “We encourage cessation and/or reduction of cannabis use during breastfeeding.”
That wording is important. “Insufficient data” does not mean safe. It means unknown.
THC in breast milk and infant exposure[12]Marijuana and Breastfeeding. Centers for Disease Control and Prevention. CDC, 2024. https://www.cdc.gov/breastfeeding-special-circumstances/hcp/vaccine-medication-drugs/marijuana.html
The strongest point in this area is also the simplest: THC is lipophilic. It dissolves readily into fat, and breast milk contains fat. That is why cannabis exposure is not comparable to a fleeting blood level that disappears after the subjective effects wear off. The U.S. Centers for Disease Control and Prevention states in its 2024 breastfeeding guidance that breast milk can contain THC “for up to 6 days after use, according to one study,” and adds that “other studies have noted even longer duration.”
So the common idea that a parent can “pump and dump” for a few hours after using cannabis and thereby avoid infant exposure is not supported by the pharmacology. Alcohol clears quickly and predictably. THC does not. Frequency of use matters, dose matters, route matters, product potency matters, and body fat stores matter. A person using a high-potency concentrate every day is not in the same exposure category as someone who used a lower-dose product once, but both can transfer THC into milk.
Researchers have tried to estimate how much of the maternal dose reaches the infant, often using a “relative infant dose” approach, but those calculations vary and rest on assumptions that are shaky in real life. Milk concentrations differ from one feeding to the next. Products sold as cannabis are not standardized across states or manufacturers. Labels can be wrong. Older studies examined lower-potency products than those commonly used now. And many studies rely on self-report, which is vulnerable to underreporting, especially in a legal environment where, as STAT reported in 2026, pregnant people and new parents can still face child welfare investigations or criminal penalties for cannabis use despite broader legalization.
There is also a second exposure pathway that gets less attention. If cannabis is smoked or vaped around an infant, exposure is not only through milk. There can be secondhand inhalation and contamination of the caregiving environment. That does not mean every measurable trace produces clinical harm. It does mean that “I only use after feeding” is not a complete risk-control strategy.
CBD adds another layer of uncertainty, not a safety exception. Some parents assume cannabidiol is different enough from THC to be acceptable while breastfeeding. Clinical guidance does not support that leap. CBD products may contain THC, pesticides, solvents, or other contaminants, and there is little high-quality lactation data for purified or commercial CBD products. Public-health advice generally treats these products cautiously for that reason.
Short-term infant effects and developmental uncertainty
The hardest question for families is the most practical one: what happens to the baby? The honest answer is that the clinical signal is concerning, but the evidence is limited and often messy.
Short-term effects reported in the literature have included sedation, poor sucking, and changes in feeding or alertness, but the data are sparse and often come from small studies, case reports, or studies where prenatal exposure cannot be separated cleanly from postnatal exposure through milk. That distinction matters. A baby exposed in utero and then through breast milk is not the same as a baby exposed only after birth. Yet many studies combine or blur those groups.[13]Persistence of Δ-9-Tetrahydrocannabinol in Human Breast Milk. E.M. Wymore, A. Palmer, J. Wang, et al.. JAMA Pediatrics, 2021. https://jamanetwork.com/journals/jamapediatrics/fullarticle/2778764
One often-cited study by Wymore and colleagues, published in 2021, found that THC could be detected in breast milk for prolonged periods among postpartum cannabis users, reinforcing that infant exposure can persist beyond the immediate period after use. What that study did not settle was downstream clinical impact. Detectable THC is not the same thing as measured injury. But neither is it harmless by default.
When developmental outcomes have been studied, interpretation becomes even harder. Infants and children exposed to cannabis during pregnancy have, in some studies, shown differences in attention, executive function, behavior, or growth. But breastfeeding-specific evidence is much thinner than pregnancy evidence, and many datasets cannot isolate lactational exposure from prenatal exposure, tobacco use, alcohol use, stress, nutrition, prematurity, and socioeconomic adversity. Those are not minor confounders. They are central ones.
This is why careful sources use language like association, signal, or uncertainty rather than making absolute claims. The CDC’s 2024 wording is restrained but clear: chemicals in cannabis, “in particular, tetrahydrocannabinol or THC,” pass through the parent’s system to the baby and “may harm your baby’s development.” “May” is doing real work there. It reflects concern without pretending the exact magnitude of risk is nailed down.
That uncertainty should not be mistaken for a green light. The infant brain is developing rapidly. Cannabinoid signaling is involved in neurodevelopment. Exposure during this period is biologically plausible as a risk, even if the literature has not yet pinned down a precise effect size for breastfeeding exposure alone. When professional groups discourage cannabis during lactation, they are acting on that combination of pharmacology, developmental vulnerability, and incomplete outcome data.
How breastfeeding benefits complicate risk communication
This is where blunt messaging can backfire. Breastfeeding is associated with lower infant infection risk, lower rates of some gastrointestinal and respiratory illnesses, and benefits for maternal health and bonding. For some families, especially those with limited formula access, unstable housing, or little postpartum support, stopping breastfeeding is not a small or simple intervention. It can create its own harms.
That is why good clinical counseling does not sound like social media certainty. It starts with the recommendation to avoid cannabis during lactation. The recommendation is firm. AAP discourages maternal marijuana use while breastfeeding. ACOG discourages it. The Academy of Breastfeeding Medicine encourages cessation or reduction. But these groups also do not frame every encounter as a reason to sever breastfeeding support, shame the parent, or trigger punishment.
The distinction matters even more because punitive systems distort disclosure. If patients fear that admitting cannabis use will bring child welfare scrutiny, they may avoid prenatal or postpartum care, underreport use, or receive no counseling at all. STAT’s 2026 reporting captured the contradiction well: legalization has expanded, but protection from investigation and criminalization has not reliably followed. Public health suffers when patients have to choose between honesty and safety.
So what should clinicians actually say? First, avoid cannabis while breastfeeding if possible. Second, if a parent is using cannabis, stopping or reducing use is better than continuing heavy use. Third, timing feeds around use is not a dependable fix because THC can remain in milk for days, not hours. Fourth, smoke and vapor exposure around the infant should be avoided. Fifth, if cannabis is being used for nausea, sleep, anxiety, or pain, offer alternatives rather than leaving the patient with a warning and no plan.
Breastfeeding counseling priorities
- Recommend avoidance Avoid cannabis while breastfeeding if possible.
- Support reduction if needed If a parent is using cannabis, stopping or reducing use is better than continuing heavy use.
- Do not rely on timing alone Timing feeds around use is not dependable because THC can remain in milk for days.
- Avoid smoke or vapor around the infant Secondhand exposure adds to milk exposure.
- Treat the reason for use Offer alternatives for nausea, sleep, anxiety, or pain instead of leaving the patient with only a warning.
The key communication challenge is to avoid two mistakes at once. One is false reassurance: “we don’t really know, so it’s probably fine.” The other is a blanket claim that breastfeeding must always stop immediately in every circumstance, regardless of the parent’s level of use, the infant’s needs, and the availability of support. The evidence does not justify the first mistake, and the realities of infant feeding make the second too crude.
A careful bottom line looks like this: THC gets into breast milk, can remain there for days, and may affect the infant, but the exact dose-response relationship and long-term clinical impact are still not well defined. That is enough for major medical organizations to advise against cannabis use during breastfeeding. It is not enough to pretend the only responsible response is moral panic or automatic family separation. The better standard is clear counseling, non-punitive support, and honesty about what medicine knows and what it still does not.
Why the research is mixed: the methodological problems readers rarely see
If readers come away from this literature confused, that is not because the question is trivial. It is because the underlying evidence is hard to produce and easy to misread. Public guidance from ACOG, the AAP, the CDC, and the Academy of Breastfeeding Medicine is fairly consistent: avoid cannabis during pregnancy, and avoid or reduce it during breastfeeding. ACOG’s 2017 Committee Opinion No. 722, reaffirmed in 2021, states that pregnant patients “should be encouraged to discontinue marijuana use,” and the CDC’s 2024 pregnancy guidance says THC and other chemicals “pass through your system to your baby and may harm your baby’s development.” But those same institutions also acknowledge major evidence gaps, especially during lactation. That combination—clear clinical caution, incomplete causal proof—can look contradictory unless you understand how this research is actually done.
How to read evidence terms in this article
- Mixed
- The literature contains concern signals and uncertainty at the same time; it does not mean safe.
- Confounding
- A distortion that occurs when cannabis use is linked to other factors, such as tobacco use or poverty, that also affect outcomes.
- Misclassification
- An exposure-measurement error, such as when people who used cannabis are recorded as non-users because of underreporting.
Evidence literacy matters here. “Mixed” does not mean “safe.” It also does not mean every observed association is proven harm caused only by cannabis. Both errors show up in public discussion all the time.
Confounding, co-use, and misclassification
Residual confounding Confounding that remains even after statistical adjustment because key exposures or social factors were measured incompletely or not measured at all.
The biggest problem is that cannabis exposure in pregnancy rarely occurs in a clean, isolated, laboratory-friendly way. Many pregnant users also smoke cigarettes, vape nicotine, drink alcohol, use other substances, experience unstable housing, have limited access to prenatal care, or are coping with severe nausea, chronic pain, anxiety, or trauma. Each of those factors can affect fetal growth, preterm birth risk, infant outcomes, or later child development on its own.
So when a study finds that prenatal cannabis exposure is associated with lower birth weight or more NICU admissions, the next question is immediate: compared with whom, and after adjusting for what? Some older studies did a poor job separating cannabis from tobacco. That matters because tobacco is strongly linked to fetal growth restriction. If a cannabis-exposed group contains a high proportion of cigarette smokers, and smoking is not fully measured or adjusted for, cannabis risk can be exaggerated. The same goes for alcohol and other drugs.
The reverse problem also happens. If exposure is measured only by self-report, cannabis use is often undercounted. SAMHSA reported in 2020 that past-month marijuana use among pregnant women aged 15 to 44 was 3.0 percent overall, with 5.7 percent in the first trimester, 3.3 percent in the second, and 1.8 percent in the third. Those figures likely miss some real use. Why would a pregnant patient underreport? Fear. Not abstract fear, either. STAT reported in 2026 that, despite legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use. When disclosure can trigger surveillance or punishment, self-report becomes less reliable. Some people deny use. Others stop reporting after the first prenatal visit. That misclassification can make exposed participants look unexposed, which tends to dilute observed effects and underestimate risk.
Timing is another source of blur. A person who used cannabis before realizing they were pregnant is often grouped with someone who used daily through all three trimesters. Those are not biologically equivalent exposures. Early first-trimester use raises one set of questions; continued heavy use late in pregnancy raises another. Yet many datasets collapse them into a binary yes/no variable. That flattening can hide dose-response patterns and make real risks harder to detect.
Breastfeeding research has the same problem, plus one more. Infants are not exposed only through milk if the mother is also using during pregnancy or through secondhand smoke after birth. When later infant behavior or sleep is measured, researchers may struggle to isolate postnatal milk exposure from prenatal exposure or shared environmental factors. ACOG in 2017 and the AAP in 2018 both said the lactation data are insufficient. That is not a claim of safety. It is a statement about uncertainty.
Potency changes and product heterogeneity
| Method problem | Why it matters |
|---|---|
| Co-use with tobacco, alcohol, or other drugs | Makes it hard to isolate a cannabis-specific effect. |
| Underreporting due to fear of punishment | Can misclassify exposed patients as unexposed and dilute observed effects. |
| Yes/no exposure categories | Collapse light early use and persistent heavy use into the same group. |
| Potency changes over time | Older cohorts may not reflect modern high-THC products. |
| Route heterogeneity | Smoking, vaping, edibles, and concentrates create different exposure patterns. |
| Lactation overlap with prenatal exposure | Breastfeeding studies often cannot separate milk exposure from in-utero exposure. |
Another reason older studies and newer headlines often fail to line up is simple: cannabis in 1995 is not cannabis in 2025. Average THC concentrations in commercial products have increased sharply over time, and product categories have multiplied. Flower, concentrates, edibles, oils, vapes, tinctures, and hemp-derived products can differ dramatically in THC dose, CBD content, contaminants, onset time, and duration of effect.
That creates a comparability problem. If a long-running cohort study enrolled pregnant participants when lower-potency smoked cannabis was common, its findings may not cleanly predict outcomes for someone using high-THC concentrates or repeated edible doses. THC is lipophilic, crosses the placenta, and is excreted into breast milk. The CDC’s 2024 breastfeeding guidance says milk can contain THC for up to 6 days after maternal use, and some studies have found longer durations. But even that statement does not answer the practical question most patients ask: how much infant exposure follows a specific product, dose, and route? For many real-world scenarios, the data are thin.
Route matters. Smoking introduces combustion byproducts. Vaping changes inhalation patterns and may involve additives. Edibles often lead to delayed onset and accidental redosing, which can increase total intake. Topicals may have very different systemic absorption. Studies that record only “marijuana use: yes/no” erase all of this.
Composition matters too. A product labeled “cannabis” may contain mostly THC, a mix of THC and CBD, or variable amounts of minor cannabinoids and terpenes. Some illicit or poorly regulated products may also contain pesticides, heavy metals, or residual solvents. If an adverse outcome is linked to “cannabis use,” what exactly caused it—the THC, another constituent, smoke exposure, a contaminant, or the conditions associated with use? The literature often cannot say.
This heterogeneity can push estimates in either direction. If a study groups very light and very heavy users together, the average effect may look small even if high-dose use carries meaningful risk. On the other hand, if a sample is drawn from a high-risk clinical population using potent products frequently, the resulting estimate may not generalize to occasional first-trimester use. Broad claims built on narrow exposure definitions are a common source of confusion.
Ethics, randomized trials, and the limits of observational science
The strongest reason the evidence will never look like a drug trial is that an actual randomized exposure trial would be unethical. Researchers cannot assign pregnant people to use THC, continue smoking cannabis, or consume cannabis while breastfeeding just to see what happens to the fetus or infant. That is why this field is dominated by observational studies: cohorts, case-control studies, registries, medical-record analyses, and follow-up of existing populations.
Observational science can be valuable. It is how medicine learned a great deal about alcohol, tobacco, certain medications, and environmental exposures in pregnancy. But it comes with limits. People choose their own exposures. Researchers measure those choices after the fact. Confounders are never captured perfectly. Statistical adjustment helps, but it cannot turn an observational association into pure causation.
That is why careful writers distinguish among an association, a signal, and established harm. Lower birth weight after prenatal cannabis exposure has shown up often enough to be concerning. Possible links to preterm birth, NICU admission, and later differences in attention, executive function, or behavior are also persistent enough that dismissing them would be irresponsible. At the same time, effect sizes vary across studies, and some findings weaken after controlling for tobacco, alcohol, income, stress, or maternal mental health.
This is also why professional guidance does not wait for impossible certainty. ACOG, the AAP, CDC, and the Academy of Breastfeeding Medicine all advise counseling, screening, and non-punitive support rather than reassurance based on weak evidence. The Academy of Breastfeeding Medicine’s 2023 Protocol #21 says, “We encourage cessation and/or reduction of cannabis use during breastfeeding.” That wording reflects both concern and the limits of the data.
Readers should keep two ideas in view at once. First, the evidence base is mixed, just as STAT wrote in 2026. Second, mixed evidence in this case sits on top of biologic plausibility—THC crosses the placenta and enters milk—and repeated observational signals that are worrying enough to justify caution. The research is messy. The clinical advice is still clear.
The legal landscape: screening, reporting, and child welfare
The legal risk of using cannabis during pregnancy is often badly misunderstood. A person may live in a state where adult use is legal, buy from a regulated store, and still face hospital reporting, child welfare scrutiny, or even criminal consequences once pregnancy enters the picture. That tension is not hypothetical. STAT reported in 2026 that “despite expanding cannabis legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use.” That is the core legal fact readers need first. Legalization changed access for adults. It did not create a safe harbor for pregnancy.
This matters because the medical evidence is neither simple nor empty. STAT also reported in 2026 that “the evidence on cannabis use in pregnancy remains mixed.” Mixed does not mean reassuring. Mainstream medical guidance remains clear: avoid cannabis during pregnancy and lactation. ACOG’s Committee Opinion No. 722, issued in 2017 and reaffirmed in 2021, states that “women who are pregnant or contemplating pregnancy should be encouraged to discontinue marijuana use.” The CDC in 2024 put it more bluntly: THC and other cannabis chemicals pass to the fetus and “may harm your baby’s development.” But when law treats every positive test as proof of child endangerment, it turns an area of uncertain evidence and individualized care into a pipeline for punishment.
How pregnancy changes the legal meaning of cannabis use
Outside pregnancy, cannabis use is usually governed by state drug law, workplace rules, housing restrictions, and impaired-driving law. Pregnancy adds a second layer: family regulation. The same conduct can be reclassified by hospitals, courts, or child welfare agencies as evidence of neglect, abuse, or prenatal endangerment. That shift is why legalization has not solved the problem.
Some states define prenatal substance exposure in child welfare statutes; others leave it to hospital policy, agency interpretation, or judicial practice. In one jurisdiction, a positive maternal or newborn toxicology screen may trigger a mandated report. In another, reporting may depend on signs of withdrawal, evidence of harm, or clinician judgment. Cannabis may be treated differently from opioids in formal policy, but in practice a THC-positive result can still start an investigation.
Testing practices sit at the center of this. Many pregnant patients assume they will be screened only if they consent. That is not always true. Clinics may ask about substance use as part of routine prenatal intake, and hospitals may order toxicology testing during labor, after delivery, or on the newborn if staff suspect exposure, if there was limited prenatal care, or if prior records mention substance use. Urine testing is common, though it has obvious limits: THC metabolites can remain detectable long after intoxication has passed, especially with frequent use, so a positive result does not show when use occurred, how much was used, or whether the infant was clinically affected. Meconium or umbilical cord testing can extend the window further.
That is where legal categories outrun science. A positive test is often treated as a hard fact. It is not. It can show exposure. It cannot, by itself, establish impairment during pregnancy, parenting capacity, or neonatal injury. Yet a lab result can carry more weight in a reporting system than the full clinical picture.
Race and class shape how this works. Drug use during pregnancy is not unique to any one group, but surveillance is not evenly distributed. Patients who rely on publicly funded hospitals, present late to care, have prior child welfare involvement, or are already viewed as “high risk” are more likely to be screened, tested, and reported. That means the legal meaning of cannabis use is not just about the substance. It is also about who gets watched.
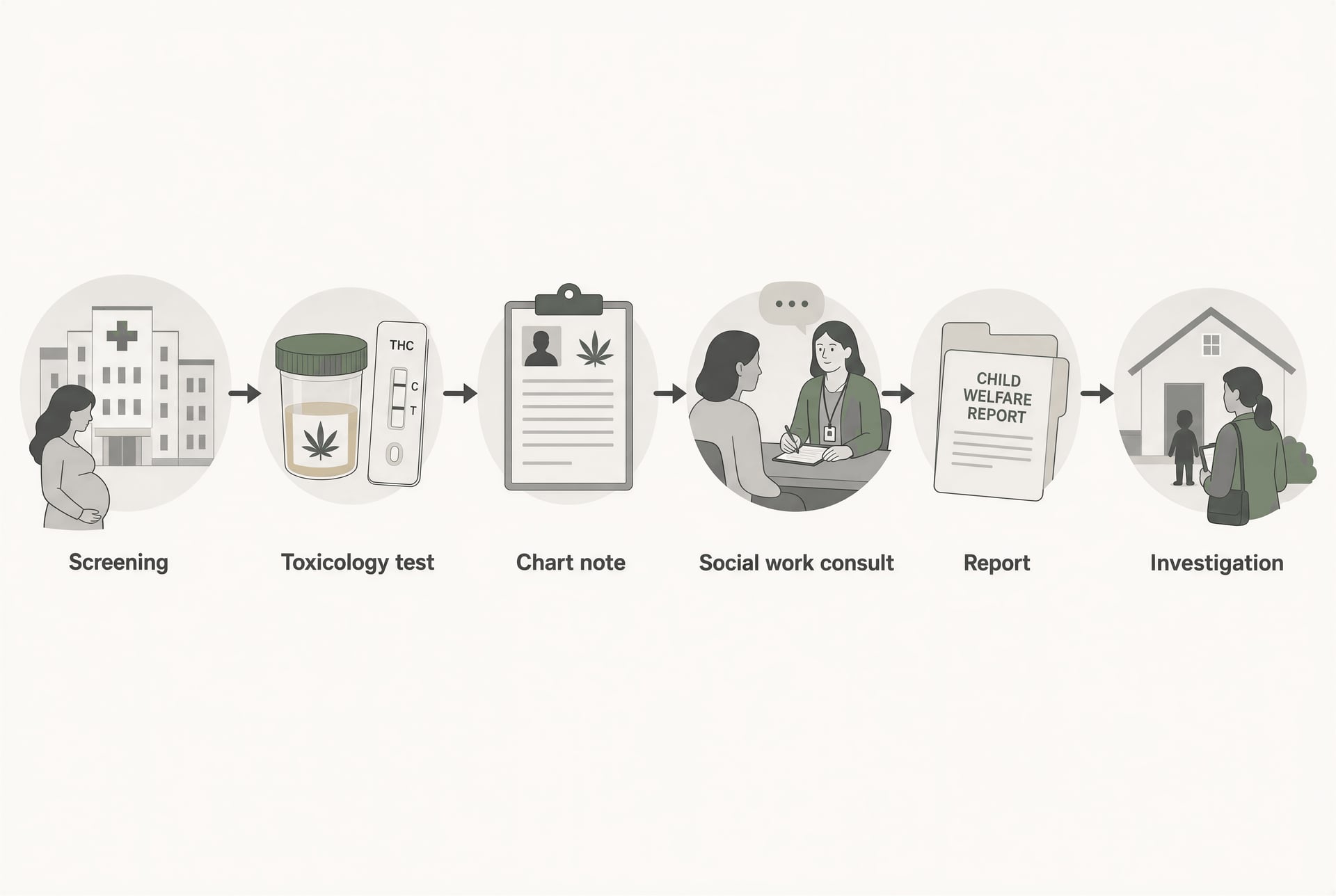
Mandatory reporting and CPS investigations
Mandatory reporting rules vary sharply by state, and that variability is one reason blanket advice about “your rights” can be misleading. Some states explicitly require health care providers to notify child protective services when an infant is born “affected by” substance exposure or withdrawal. Others require the creation of a Plan of Safe Care under federal child welfare law, especially after the Child Abuse Prevention and Treatment Act amendments, without necessarily defining every exposure as abuse. Some states include cannabis in practice even if their statutes focus on controlled substances more generally. Others carve out medical cannabis in limited contexts, but those carve-outs may not stop a hospital from making a report.
How a disclosure can become a child-welfare case
- Disclosure or suspicion A patient report, chart history, or clinician concern can prompt testing.
- Testing Maternal or newborn toxicology may be ordered during pregnancy, labor, or after delivery.
- Social work consult A positive result often triggers additional evaluation.
- Report Hospital staff may make a child-protection report depending on state law or policy.
- Investigation CPS may open a case even if no court petition is filed.
The practical sequence often looks like this: disclosure or suspicion leads to testing; testing leads to a social work consult; the consult may lead to a report; the report may open a CPS investigation even if no petition is ever filed in court. For families, that distinction matters less than policymakers think. An investigation can mean home visits, interviews, safety plans, demands for follow-up testing, and scrutiny of older children in the household.
Not every report produces removal. Many do not. Still, the investigation itself is a state intervention with real costs. Parents may need lawyers. They may be told to complete treatment they do not clinically need. They may feel pressure to stop breastfeeding immediately after a positive THC screen, even though lactation guidance is not framed through automatic family separation. ACOG says there are “insufficient data” on effects during lactation and therefore marijuana use is discouraged. The American Academy of Pediatrics said in 2018 that the data are insufficient and maternal use while breastfeeding is discouraged. The Academy of Breastfeeding Medicine’s 2023 Protocol #21 takes a counseling approach and says, “We encourage cessation and/or reduction of cannabis use during breastfeeding.” None of those statements says that a positive test automatically equals neglect. Child welfare systems often move as if it does.
The postpartum setting raises the stakes because newborn testing can bring legal exposure even when prenatal care was otherwise stable. A patient may have stopped using weeks before delivery and still test positive, or the infant’s specimens may reflect past exposure without immediate clinical illness. Yet once the report is made, families enter a system that is difficult to exit quickly.
Why punitive policy can undermine prenatal care
Punitive policy is often defended as fetal protection. The public-health case against it is strong. If people think disclosure will trigger police contact, CPS referral, or loss of custody, they are less likely to answer screening questions honestly and more likely to avoid prenatal care altogether. That is not speculation; it follows from basic incentive structure. When the system treats admission as self-incrimination, silence becomes rational.
That is dangerous because pregnancy is exactly when clinicians need accurate information. Cannabis use may interact with nausea, mental health symptoms, polysubstance use, or unstable housing. A patient using cannabis daily in the first trimester may also be struggling with vomiting, trauma, nicotine dependence, or inability to access safer treatments. SAMHSA reported in 2020 that past-month marijuana use among pregnant women aged 15 to 44 was 3.0 percent overall, with a higher 5.7 percent in the first trimester, then 3.3 percent in the second and 1.8 percent in the third. Self-report probably understates actual use. If fear drives that reporting even lower, clinicians lose a key chance to counsel, taper, treat nausea with better-studied options, and address other risks.
The major professional bodies have largely converged on the same answer: screen, counsel, support, do not punish. ACOG recommends asking all women about substance use before and early in pregnancy, but it also says the purpose of screening is treatment, not punishment. That distinction is not semantic. It is the difference between prenatal care as a doorway and prenatal care as surveillance.
Punishment also distorts lactation counseling. CDC guidance from 2024 says breast milk can contain THC for up to 6 days after maternal use, and some studies have found longer durations. That supports advising against cannabis use while breastfeeding. It does not support reflexive coercion that scares mothers away from postpartum care, pediatric follow-up, or lactation help. Public-health messaging works best when it is credible about uncertainty and clear about concern: THC reaches the fetus and breast milk; some studies link prenatal exposure with lower birth weight, possible preterm birth, NICU admission, and later problems in attention or behavior; confounding remains substantial; avoidance is the safest recommendation. That message is medically defensible. Threats are not a substitute for it.
The bottom line is uncomfortable but plain. Pregnancy can turn legal adult cannabis use into evidence for state scrutiny. Reporting rules differ, testing is uneven, and marginalized patients bear more of the burden. Policies built around punishment may look tough, but they can push people away from the very prenatal and postpartum care most likely to reduce harm.
How clinicians should talk with patients
Core steps for clinicians
- Ask routinely Use universal, non-shaming screening rather than selective suspicion-based questioning.
- Explain the evidence honestly THC crosses the placenta and enters breast milk; the literature is mixed but concerning enough that avoidance is recommended.
- Offer alternatives Treat the symptom or stressor that made cannabis seem useful, such as nausea, insomnia, anxiety, or pain.
The clinical task is straightforward to state and harder to do well: ask every pregnant and postpartum patient about cannabis in a routine, non-shaming way; explain that major medical groups advise avoiding it during pregnancy and breastfeeding; and then offer realistic help for the symptoms or stressors that led to use in the first place. That approach fits both the evidence and the ethics. Scare tactics do not. Neither do legal threats. As STAT reported in 2026, “despite expanding cannabis legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use,” a reality that can push people away from prenatal care rather than toward safer care.

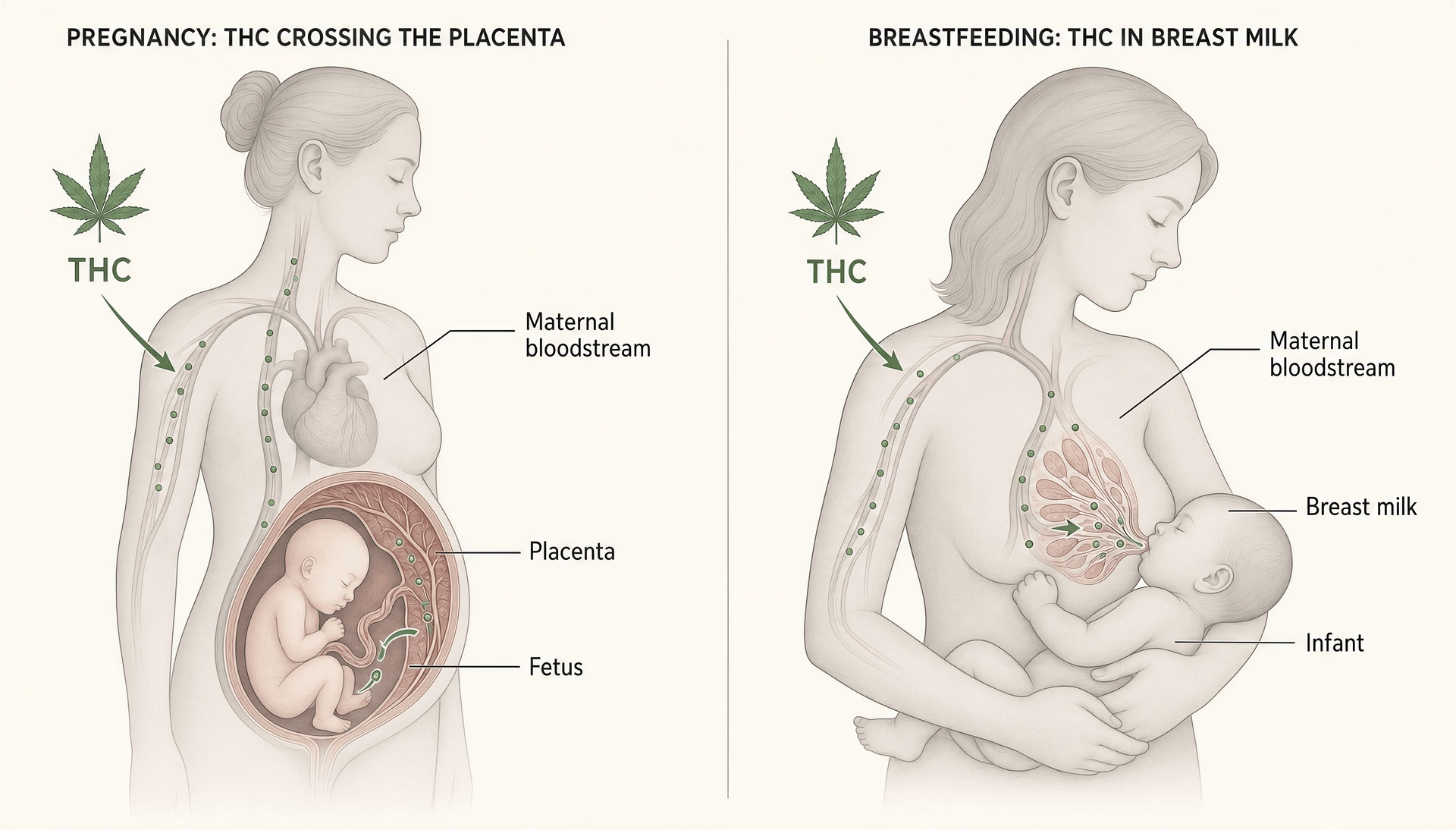{kind=link}
{kind=link}
{kind=link}
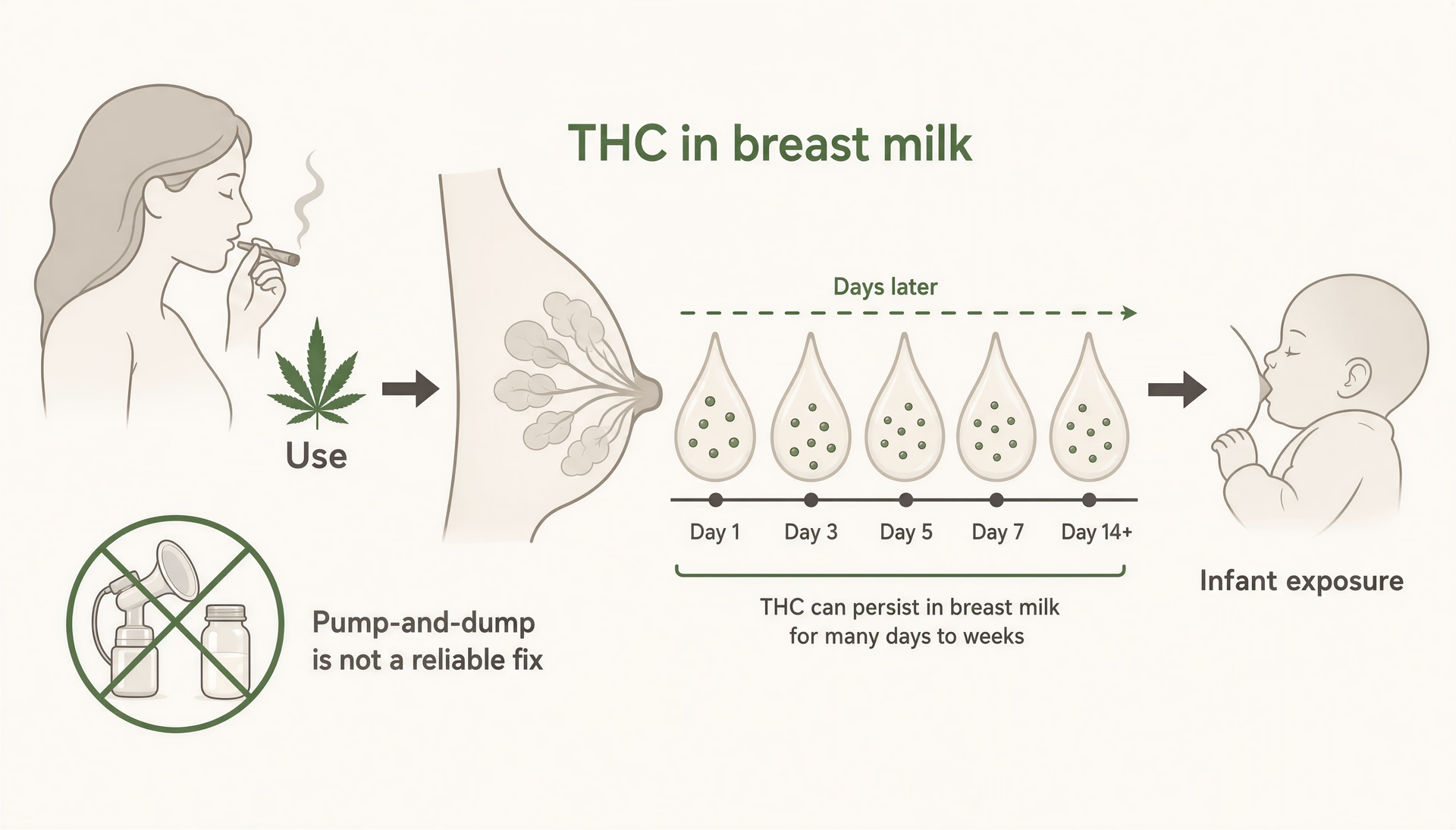{kind=link}
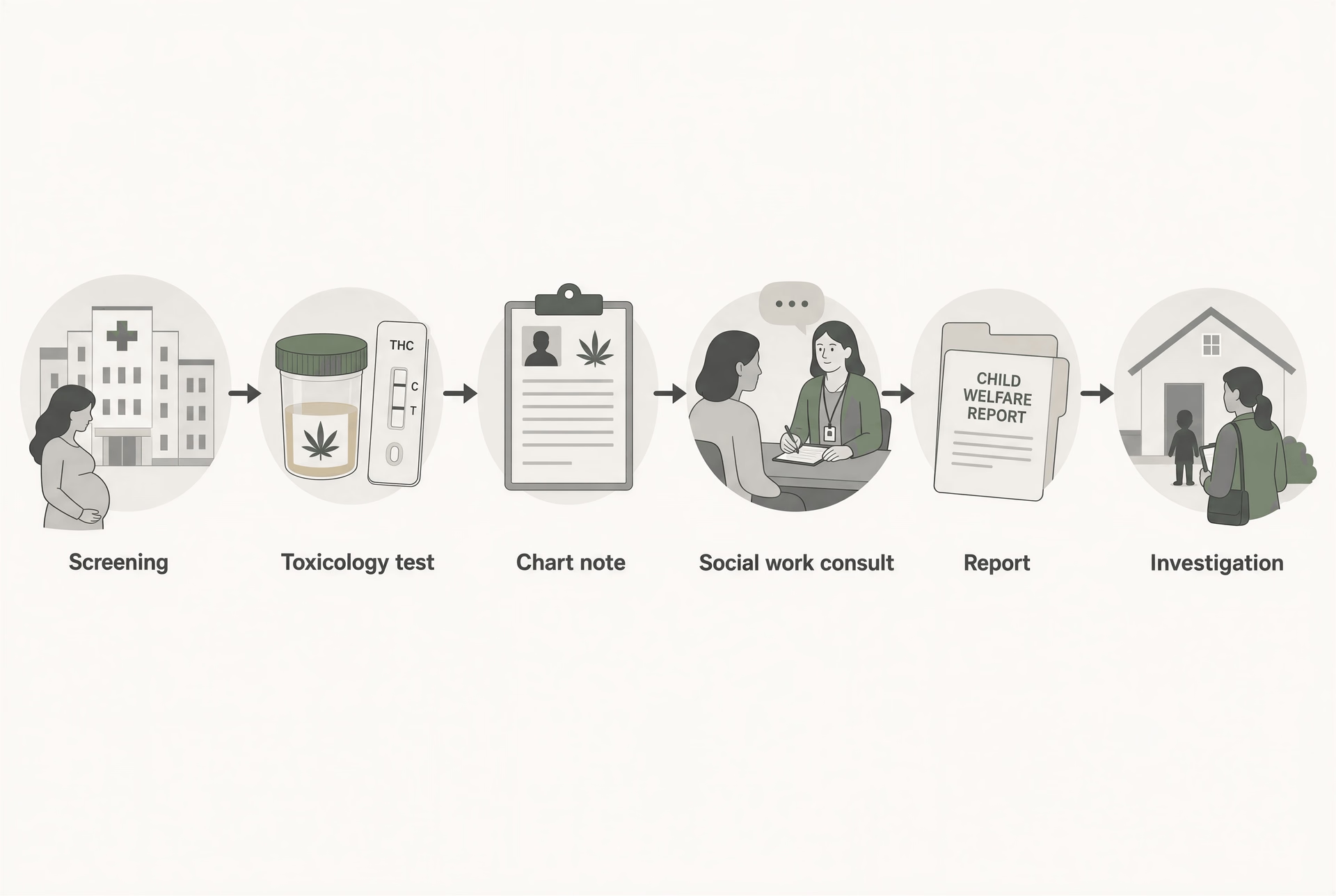{kind=link}
{kind=link}
Nonjudgmental screening and informed consent
Screening works best when it is universal. Not selective. If a clinician only asks younger patients, poorer patients, or patients who “seem high,” the process becomes stigma dressed up as medicine. ACOG’s Committee Opinion No. 722, first issued in 2017 and reaffirmed in 2021, supports asking all women before and in early pregnancy about tobacco, alcohol, other drugs, and marijuana use. The point is clinical care, not punishment.
How that conversation starts matters. “Many people use cannabis for nausea, sleep, anxiety, pain, or appetite. Have you used any THC, marijuana, delta-8, CBD, or edibles since becoming pregnant or while breastfeeding?” is better than “You’re not using drugs, are you?” The first question acknowledges common reasons for use and names products patients may not think of as “marijuana.” That matters because product labels are inconsistent, potency has changed over time, and patients often assume vaping, edibles, or CBD-heavy products are safer.
Patients also deserve plain-language informed consent. Not a lecture. Something like this is accurate: THC is lipophilic, crosses the placenta, and gets into breast milk. The CDC said in 2024 that chemicals in cannabis, “in particular, tetrahydrocannabinol or THC,” pass to the baby and may harm development. The CDC also states that breast milk can contain THC for up to 6 days after use, with some studies finding longer duration. ACOG advises that pregnant patients should be encouraged to discontinue marijuana use, and it discourages use during lactation because the data are insufficient to declare it safe. The AAP took a similar position in 2018, and the Academy of Breastfeeding Medicine in Protocol #21, revised in 2023, encourages cessation or reduction during breastfeeding.
That message should be honest about uncertainty without becoming falsely reassuring. The evidence in pregnancy is mixed, as STAT noted in 2026, but “mixed” does not mean “no concern.” Research has linked prenatal cannabis exposure with lower birth weight and signals for preterm birth, NICU admission, and later differences in attention, behavior, or executive function. At the same time, many studies are hard to interpret because cannabis use often travels with tobacco exposure, alcohol, poverty, chronic stress, undernutrition, and changing product potency. So the right clinical sentence is not “we know this causes severe harm in every case,” and not “we don’t really know, so it’s probably fine.” It is: there are enough concerning signals, and too little evidence of safety, that avoidance is the safest recommendation.
Clinicians should also explain confidentiality and its limits before screening, especially in places where drug testing can trigger reporting. Patients are more likely to tell the truth when they know what will happen with the information. If state law or hospital policy creates reporting obligations, that should be disclosed clearly, not sprung on a patient after a positive test. Evidence-based counseling cannot function if the patient reasonably expects that honesty will be used against them.
Counseling for symptom relief without cannabis
A lot of cannabis use in pregnancy is self-treatment. SAMHSA reported in 2020 that past-month marijuana use among pregnant women ages 15 to 44 was 3.0 percent overall, but 5.7 percent in the first trimester, when nausea and vomiting are often worst. If clinicians want people to stop, they need to treat the symptom that made cannabis seem useful.
Symptom-focused alternatives clinicians can discuss
- Nausea and vomiting Small frequent meals, ginger if tolerated, vitamin B6, doxylamine-pyridoxine, and escalation for severe vomiting or hyperemesis.
- Sleep Regular bedtime, limit late caffeine, reduce screen exposure, and address reflux, pain, restless legs, or anxiety.
- Anxiety Assess for panic, trauma, unsafe housing, or depression; consider therapy, social work support, and medications with better pregnancy data when indicated.
- Pain Physical therapy, heat or ice when appropriate, stretching, support belts, massage, acetaminophen when suitable, and specialty input for refractory pain.
For nausea and vomiting, the conversation can be practical: eat small frequent meals, try ginger if tolerated, consider vitamin B6, and discuss doxylamine-pyridoxine or other pregnancy-appropriate antiemetics when needed. If the patient says cannabis is the only thing that works, that is a cue to escalate care, not argue. Severe vomiting may need dehydration assessment, medication adjustment, or evaluation for hyperemesis gravidarum.
For sleep, start with basics that are easy to try and easy to abandon if they fail: regular bedtime, limiting late caffeine, reducing screen exposure, and addressing reflux, restless legs, pain, or anxiety that may be driving insomnia. Sedative substitutions should not be casual; pregnancy-safe options depend on the clinical picture. The key is not simply “don’t use cannabis,” but “here is what we can do instead.”
For anxiety, clinicians should resist reducing everything to willpower. Ask what the patient is experiencing: panic, trauma symptoms, racing thoughts, unsafe housing, intimate partner violence, or simple overwhelm. Brief counseling, psychotherapy referral, mindfulness-based strategies, social work support, and when indicated, medications with better pregnancy data than THC are all on the table. Untreated anxiety also carries risks. Patients need that acknowledged.
Pain is similar. Back pain, pelvic girdle pain, migraines, and chronic pain conditions are common reasons for cannabis use. Safer paths may include physical therapy, heat or ice when appropriate, stretching, support belts, massage, acetaminophen when suitable, and specialty input for refractory pain. A patient who feels heard is more likely to try alternatives. A patient who feels judged may nod and keep using.
Breastfeeding counseling needs its own careful framing. The Academy of Breastfeeding Medicine’s 2023 protocol does not treat every exposure the same, and that is useful. For a parent with occasional use, counseling may focus on cessation or reduction, avoiding secondhand smoke exposure, and discussing the unknowns. For heavy daily use, stronger advice and more support are warranted. But “pump and dump” is not a reliable fix for THC, because THC can persist in milk for days rather than hours.
When substance use disorder treatment may be needed
When cannabis use may need substance-use treatment support
- Daily or near-daily use
- Inability to cut down
- Withdrawal symptoms such as irritability or insomnia
- Prioritizing use over eating or appointments
- Using despite social or medical harms
- Rapid return to use after trying to stop
Not every prenatal cannabis use pattern is a substance use disorder. Some patients can stop after one conversation. Others cannot, and clinicians should be prepared for that without turning the encounter into a moral trial. Warning signs include daily or near-daily use, inability to cut down, withdrawal symptoms such as irritability or insomnia, prioritizing use over eating or appointments, using despite social or medical harms, and returning to use quickly after trying to stop.
At that point, brief advice is not enough. Referral pathways should be concrete: addiction medicine, perinatal behavioral health, social work, outpatient treatment, and psychiatric care when anxiety, depression, trauma, or other disorders are tangled up with use. Motivational interviewing often works better than confrontation. So does frequent follow-up. “What would make cutting back possible this week?” can move care forward more than “You have to stop.”
One more point matters. Punitive responses are bad medicine. Legal threats may produce silence, missed visits, or avoidance of hospital care. They do not create informed consent, symptom control, or recovery. The better standard is universal screening, clear advice to avoid cannabis, symptom-focused alternatives, and treatment access when stopping is hard. That is what evidence-based care looks like here.
What patients can do if they are pregnant, trying to conceive, or breastfeeding
What patients can do now
- Disclose use clearly Tell your clinician what product you use, how often, how much, and why you use it.
- Ask for help with the reason you use it Seek treatment for nausea, sleep problems, anxiety, pain, or appetite loss rather than self-treating with cannabis.
- Work toward stopping If immediate abstinence is hard, reduction can be a step, but it is not proof of safety.
- Do not rely on labels CBD products may contain THC or contaminants, and potency varies.
- Keep care on track Stay engaged with prenatal, postpartum, pediatric, and lactation care rather than avoiding care out of fear.
If you are pregnant, planning pregnancy, or breastfeeding, the clearest public-health message is still to avoid cannabis if you can. That is the position of the American College of Obstetricians and Gynecologists, which states that women who are pregnant or contemplating pregnancy should be encouraged to discontinue marijuana use, and of the American Academy of Pediatrics and CDC, which also discourage use during breastfeeding. That recommendation does not mean every exposure causes harm. It means the balance of concern runs in one direction, while the evidence is messy enough that no responsible clinician can promise safety.
That distinction matters, because fear and punishment can make people hide use or avoid care. STAT reported in 2026 that legalization has not shielded pregnant patients from child welfare investigations or criminal penalties, even though “the evidence on cannabis use in pregnancy remains mixed.” Patients need plain facts, not panic. THC crosses the placenta. It is fat-soluble, so it also moves into breast milk and can persist there. CDC says breast milk can contain THC for up to 6 days after use, and some studies have found longer durations. So the practical goal is not moral purity. It is reducing fetal and infant exposure, getting accurate medical guidance, and keeping prenatal and pediatric care on track.
Stopping or reducing use safely
For many people, stopping is emotionally harder than it sounds. Cannabis may have been used for nausea, sleep, anxiety, pain, appetite, or habit. Some discover pregnancy while using daily or near-daily products with much higher THC concentrations than were common a generation ago. Others use occasionally and assume a small amount does not matter. Either way, honesty helps.
If you are trying to conceive or have just learned you are pregnant, tell your clinician what you are using: smoked flower, vaped oil, edibles, concentrates, delta-9-THC products, or products labeled CBD that may still contain THC. Include how often, how much, and why you use it. “I use a 10 mg edible every night for sleep” is more useful than “sometimes.” So is “I vape because I cannot keep food down.” Clinicians can only offer alternatives if they know what problem you were trying to solve.
Stopping suddenly is usually not medically dangerous in the way alcohol or benzodiazepine withdrawal can be, but it can still be uncomfortable. People may feel irritable, restless, anxious, nauseated, have vivid dreams, or struggle with sleep for several days to a couple of weeks. That is one reason “just quit” often fails. Ask for help with the underlying symptom. If nausea is the issue, ask about pregnancy-tested options instead of self-treating with cannabis. If anxiety or insomnia is driving use, ask about non-cannabis approaches that are considered safer in pregnancy.
Reduction is not the same as safety, but it can still matter when immediate abstinence is hard. The Academy of Breastfeeding Medicine’s 2023 Protocol #21 says it encourages cessation and/or reduction of cannabis use during breastfeeding. The same logic can help during pregnancy while someone is working toward stopping: fewer episodes, lower cumulative exposure, and avoiding high-potency concentrates likely beats repeated heavy use. But “cutting back” should be treated as a step, not proof of safety.
Do not rely on product labels to protect you. THC content varies. Some products sold as CBD contain measurable THC. Synthetic or semi-synthetic cannabinoids raise another problem: even less pregnancy and lactation data.
Questions to ask an obstetric or pediatric clinician
Questions patients can ask clinicians
- What do you recommend I do starting today, given how often I use and what form I use?
- Are there safer treatments for my nausea, sleep problem, anxiety, or pain?
- Do you do urine drug testing routinely, only with consent, or only for specific medical reasons?
- Could a positive test affect my care, my delivery hospitalization, or child welfare reporting where I live?
- If I am breastfeeding or pumping, how does my infant’s age change the discussion?
- If I used cannabis recently, what signs in my baby should prompt a call to the pediatrician?
Ask direct questions, even if you are worried about judgment. Try these:
What do you recommend I do starting today, given how often I use and what form I use? Are there safer treatments for my nausea, sleep problem, anxiety, or pain? Do you do urine drug testing routinely, only with consent, or only for specific medical reasons? Could a positive test affect my care, my delivery hospitalization, or child welfare reporting where I live? If I am breastfeeding or pumping, how does my infant’s age change the discussion? If I used cannabis recently, what signs in my baby should prompt a call to the pediatrician?
Those legal and policy questions are not paranoid. They are practical. A non-punitive approach is best for health, but policies vary by state and by hospital system. Knowing the rules in advance can reduce surprises and help patients stay engaged in care rather than disappearing from it.
For breastfeeding, ask your pediatric or lactation clinician to discuss three variables plainly: infant age, frequency of use, and route of exposure. A preterm newborn or a medically fragile infant deserves a more cautious conversation than a thriving older infant. Daily inhaled or edible THC exposure is different from a one-time use weeks ago. Smoking or vaping around the infant adds secondhand and thirdhand exposure on top of breast milk transfer.
One point should be very clear: pumping and dumping is not a reliable fix for cannabis. Unlike alcohol, THC does not clear from milk on a short clock you can predict after a single feed. Because THC is lipophilic and can remain detectable in milk for days, discarding milk right after use does not mean the next milk is THC-free.
What to do after unintentional early exposure
Many pregnancies are recognized after several weeks, and early exposure is common enough that panic is the wrong response. SAMHSA reported in 2020 that past-month marijuana use among pregnant women ages 15 to 44 was 3.0 percent overall, but 5.7 percent in the first trimester. Self-report probably misses some use, so real exposure is likely higher. You are not the only person this has happened to.
If you used cannabis before you knew you were pregnant, the next move is straightforward: stop if you can, write down roughly when and how much you used, and bring that information to prenatal care. Do not assume that because something bad could happen, something bad did happen. Evidence links prenatal exposure to signals such as lower birth weight and possible increases in preterm birth or NICU admission, and some studies suggest later differences in attention, executive function, or behavior. But those studies are often limited by tobacco and alcohol co-use, poverty, stress, and changing product potency. That is why clinicians should counsel seriously without predicting a specific outcome from a small early exposure.
What helps now is ordinary good prenatal care. Start or continue prenatal vitamins with folic acid if your clinician recommends them. Keep appointments. Get help for nausea or insomnia instead of returning to cannabis because you are scared. If you are breastfeeding and had a single unplanned use, do not make assumptions based on internet folklore; ask a pediatric clinician how to think about timing, infant age, feeding alternatives, and whether temporary interruption is being considered because of your pattern of use, not because “pump and dump” solved it.
The bottom line for patients is simple even if the evidence is not: disclose use, ask for support, avoid further exposure when possible, and seek counseling grounded in medicine rather than shame.
What remains unknown and where the next evidence should come from
The next phase of research needs to do two things at once: sharpen the biology and stop pretending biology is the whole story. Major clinical groups already advise avoiding cannabis during pregnancy and breastfeeding. ACOG states that pregnant patients “should be encouraged to discontinue marijuana use,” and the CDC warns that THC passes to the fetus and may affect development. That is the current practice baseline. But the evidence underneath those recommendations is still uneven, which is exactly why better studies matter. STAT reported in 2026 that “the evidence on cannabis use in pregnancy remains mixed,” even as patients continue to face child-welfare investigations and criminal penalties. That combination is not acceptable. If law and medicine are going to act with confidence, the data need to catch up.
Dose-response and timing of exposure
One of the biggest gaps is simple to describe and hard to fix: how much THC, at what point in gestation, produces which risks? Many published studies still sort exposure into crude categories such as “any use during pregnancy” or “self-reported past-month use.” That washes out the questions patients and clinicians actually ask. Is a single exposure at six weeks different from repeated daily use through the second trimester? Does risk rise in a straight line with dose, or is there a threshold effect? Are signals for lower birth weight driven mainly by frequent use, by co-use with tobacco, or by a subgroup with severe nausea and poor nutrition?
Timing matters because fetal development is not one event. It is a sequence. The first trimester includes organ formation and is also the period when cannabis use appears most common. SAMHSA reported in 2020 that past-month marijuana use among pregnant women aged 15 to 44 was 5.7 percent in the first trimester, versus 3.3 percent in the second and 1.8 percent in the third. That pattern may reflect recognition of pregnancy and later quitting, but it also means any study that treats all prenatal exposure as interchangeable is missing a key biological and behavioral fact.
What better pregnancy studies should measure
- Trimester-specific exposure rather than a yes/no checkbox
- THC dose in milligrams where possible
- Frequency separated from intensity
- Occasional use distinguished from persistent daily use
- Product type and route of administration
- Self-report combined with biological measures in non-punitive research settings
The research agenda here should be explicit. Studies need trimester-specific exposure measures, not a yes-or-no checkbox. They should quantify THC exposure in milligrams where possible, distinguish frequency from intensity, and separate occasional use from persistent daily use. Better still, they should combine self-report with biological measures such as blood, urine, or meconium testing, while handling those data in ways that do not trigger punishment or scare people away from care. A large prospective cohort that enrolls patients early, records product type and route of administration, and follows children over time would be more useful than another retrospective chart review with vague exposure labels.
Route of administration also deserves focused study. Inhaled cannabis produces a rapid spike in blood THC. Edibles generally have slower onset and longer duration, with different metabolites and more variable dosing. Those are not minor pharmacokinetic details. They may shape fetal exposure in very different ways. Yet many studies group smoked, vaped, and ingested products together. That made more sense twenty years ago than it does now.
CBD, minor cannabinoids, and modern high-potency products
A second major blind spot is that much of the literature does not match the market people are actually using. Older cohorts often captured exposure from lower-potency flower in periods before concentrates, high-dose edibles, and CBD-heavy products were common. Today, many patients are not using a generic “marijuana” exposure. They are using products with highly variable THC concentrations, different ratios of THC to CBD, and additional cannabinoids such as CBG or CBN. Research built on 1990s or early 2000s exposure patterns cannot answer all 2020s questions.
THC remains the compound of greatest concern because it is lipophilic, crosses the placenta, and is excreted into breast milk. But that does not mean CBD can be waved through as harmless. The evidence base on CBD in pregnancy is thin, especially for commonly used over-the-counter formulations that may contain contaminants, inaccurate labeling, or more THC than advertised. Some patients switch from THC-dominant products to CBD-dominant ones hoping they have found a safer option. Right now, that hope is not backed by enough human pregnancy data.
Future pregnancy research should separate THC-dominant, CBD-dominant, and mixed products rather than pooling all cannabis exposures together.Preliminary evidence
The next evidence should therefore separate THC-dominant, CBD-dominant, and mixed products rather than treating all cannabis-related exposure as one category. It should also account for potency. A single inhalation from a concentrate with 70 percent THC is not equivalent to a puff from flower at 12 percent THC, and a 10-mg edible is not the same as a 100-mg edible. If a study cannot estimate dose and product composition, it can still be useful, but its conclusions should stay modest.
This is also where confounding needs a more honest treatment. Potency changes do not just complicate risk estimates; they can reverse them or blur them beyond usefulness. If an older study found weak associations at lower average THC exposures, that does not reassure us about current products. It means the external validity is limited. New guidance warning against cannabis use during pregnancy, reported in 2026, reflects this reality. Clinical advice is being made under uncertainty, with concern that products have changed faster than the research.
Better lactation studies and more just policy research
Breastfeeding is where the evidence gaps become especially frustrating. Professional bodies are cautious for a reason. ACOG says data are insufficient to evaluate effects during lactation and breastfeeding, and the AAP similarly states that the data are insufficient, so maternal marijuana use while breastfeeding is discouraged. The Academy of Breastfeeding Medicine’s 2023 Protocol #21 takes a practical line: “We encourage cessation and/or reduction of cannabis use during breastfeeding.” That wording reflects uncertainty, not indifference.
What better lactation studies should answer
- Whether intermittent maternal use differs meaningfully from daily use
- How milk THC concentrations track with timing of use, product type, and maternal body composition
- Whether there are detectable effects on infant sedation, feeding, growth, sleep, or later neurodevelopment
- How outcomes differ across exclusive breastfeeding, mixed feeding, formula supplementation, cessation, and continued use at different levels
What is needed now are real-world lactation studies that move beyond the question of whether THC enters milk. We already know it does. The CDC states that breast milk can contain THC for up to 6 days after use, with some studies showing even longer duration. The harder question is what infant outcomes follow from that exposure under actual feeding patterns. Does intermittent maternal use differ meaningfully from daily use? How do milk THC concentrations track with timing of use, product type, and maternal body composition? Are there detectable effects on infant sedation, feeding, growth, sleep, or later neurodevelopment once confounding is handled carefully?
These studies need repeated milk sampling, quantified cannabinoid assays, infant exposure estimates, and follow-up that measures outcomes people care about, not only lab values. They also need comparison groups that reflect reality: exclusive breastfeeding, mixed feeding, formula supplementation, cessation during lactation, and continued use at different levels. Breastfeeding has established benefits. Research that ignores that context can mislead by framing the question too narrowly.
Then there is the policy side. It is not secondary. STAT’s 2026 reporting made clear that expanding legalization has not protected pregnant people from child welfare investigations or criminal penalties for cannabis use. That should trigger a different kind of evidence agenda: what do mandatory reporting laws, punitive screening practices, and fear of prosecution do to prenatal care attendance, disclosure of substance use, breastfeeding decisions, and maternal-infant outcomes? If patients avoid care because honesty may bring surveillance or custody threats, the research will stay biased and the harms will grow.
The best future evidence will link these threads rather than splitting them apart. Measure trimester-specific exposure. Quantify THC. Compare inhaled versus edible products. Study CBD-dominant formulations directly. Follow breastfeeding dyads in the real world. And test whether supportive, non-punitive care improves outcomes more than punishment does. The biology matters. So does the system patients have to survive while pregnant.
Key takeaways
What is reasonably established
- Established pharmacology
- THC crosses the placenta and enters breast milk
- Milk persistence
- CDC says up to 6 days after use, with longer durations reported elsewhere
- Most repeated pregnancy signal
- Lower birth weight / fetal growth restriction
- Other concerning signals
- Possible preterm birth, NICU admission, and later attention, behavior, or executive-function differences
- Main uncertainty
- Dose-response, product-specific effects, and breastfeeding-specific infant outcomes remain poorly defined
- Current guidance
- Avoid cannabis during pregnancy and breastfeeding; use non-punitive screening and counseling
Some facts are not especially controversial anymore. Delta-9-tetrahydrocannabinol, or THC, crosses the placenta and reaches the fetus. It is also excreted into breast milk. The CDC stated in 2024 that breast milk can contain THC for up to 6 days after maternal use, and some studies have reported longer detection windows. That matters because THC is lipophilic, stored in fat, and not cleared on the same timeline as a single drink.
The clinical guidance is also consistent. ACOG’s Committee Opinion No. 722, issued in 2017 and reaffirmed in 2021, says people who are pregnant or contemplating pregnancy should be encouraged to discontinue marijuana use. The AAP in 2018 discouraged maternal use during breastfeeding. The Academy of Breastfeeding Medicine’s Protocol #21, revised in 2023, encourages cessation or reduction during breastfeeding. CDC guidance says the chemicals in cannabis, especially THC, pass to the baby and may affect development.
The outcome data are less certain than the pharmacology, but not reassuring. Prenatal exposure has been linked in many studies and reviews with lower birth weight, and in some analyses with preterm birth and NICU admission. Signals also appear later in childhood, especially around attention, executive function, and behavior.
What is uncertain
The evidence base is mixed, and that phrase should not be twisted into “safe.” Many pregnancy studies struggle with confounding: tobacco use, alcohol, other drugs, nausea severity, poverty, stress, and uneven access to care. Self-report misses use. Potency has changed sharply over time, so older cohorts may not reflect current products.
Breastfeeding data are even thinner. ACOG and the AAP both say the infant effects during lactation are not well defined. That is a research gap, not a clean bill of health. Uncertainty cuts both ways.[14]National Survey on Drug Use and Health data portal. Substance Abuse and Mental Health Services Administration. SAMHSA Data, 2020. https://www.samhsa.gov/data/
Prevalence is also easy to underread. SAMHSA reported in 2020 that past-month marijuana use among pregnant women ages 15 to 44 was 3.0 percent overall, rising to 5.7 percent in the first trimester.
What current guidance advises
Current medical guidance favors screening, counseling, and non-punitive support, not scare tactics. Patients should be advised to avoid cannabis during pregnancy and breastfeeding, including for nausea relief. STAT reported in 2026 that legalization has not protected pregnant people from child-welfare investigations or criminal penalties, and those punitive responses can push people away from prenatal care. The short version is plain: the evidence is imperfect but concerning enough that major medical bodies advise against use; THC reaches the fetus and breast milk; and uncertainty is not evidence of safety.
References
- [1]Despite expanding cannabis legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use. STAT, 2026. https://www.statnews.com/2026/03/02/cannabis-laws-pregnancy-cps/
- [2]Marijuana Use During Pregnancy and Lactation. ACOG Committee Opinion No. 722, 2017. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2017/10/marijuana-use-during-pregnancy-and-lactation
- [3]Cannabis and Pregnancy. CDC, 2024. https://www.cdc.gov/cannabis/health-effects/pregnancy.html
- [4]Marijuana Use During Pregnancy and Breastfeeding: Implications for Neonatal and Childhood Outcomes. Pediatrics, 2018. https://publications.aap.org/pediatrics/article/142/3/e20181889/38625/Marijuana-Use-During-Pregnancy-and-Breastfeeding
- [5]Academy of Breastfeeding Medicine Clinical Protocol #21: Breastfeeding in the Setting of Substance Use and Substance Use Disorder. ABM Clinical Protocol, 2023. https://www.bfmed.org/protocols
- [6]Despite expanding cannabis legalization, pregnant people can still face child welfare investigations and criminal penalties for cannabis use. STAT, 2026. https://www.statnews.com/2026/03/02/cannabis-laws-pregnancy-cps/
- [7]National Survey on Drug Use and Health data portal. SAMHSA Data, 2020. https://www.samhsa.gov/data/
- [8]Prenatal exposure to cannabis and maternal and child health outcomes: a systematic review and meta-analysis. BMJ Open, 2016. https://bmjopen.bmj.com/content/6/4/e009986
- [9]Association Between Stillbirth and Illicit Drug Use and Smoking During Pregnancy. Obstetrics & Gynecology, 2014. https://pubmed.ncbi.nlm.nih.gov/24553166/
- [10]Prenatal marijuana and alcohol exposure and academic achievement at age 10. Neurotoxicology and Teratology, 2008. https://pubmed.ncbi.nlm.nih.gov/19004561/
- [11]Associations Between Prenatal Cannabis Exposure and Childhood Outcomes: Results From the ABCD Study. JAMA Psychiatry, 2020. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2765199
- [12]Marijuana and Breastfeeding. CDC, 2024. https://www.cdc.gov/breastfeeding-special-circumstances/hcp/vaccine-medication-drugs/marijuana.html
- [13]Persistence of Δ-9-Tetrahydrocannabinol in Human Breast Milk. JAMA Pediatrics, 2021. https://jamanetwork.com/journals/jamapediatrics/fullarticle/2778764
- [14]National Survey on Drug Use and Health data portal. SAMHSA Data, 2020. https://www.samhsa.gov/data/