






Why cannabis pharmacokinetics is more complicated than the standard inhaled-versus-edible cliché
A lot of public-facing cannabis education stops at a tidy contrast: inhaled THC acts fast, edibles act slow. That is broadly true, but it is not enough to explain what actually happens in the body, and it becomes misleading when people try to infer dose, timing, intoxication, or impairment from a product label, a blood draw, or a urine test. A useful opening frame came from a 2019 Nature Medicine news feature on cannabidiol. Even as CBD products were spreading rapidly, the piece reported that researchers were still trying to sort out cannabidiol’s absorption, distribution, and metabolism, exposing a gap between consumer use and scientific certainty (Nature Medicine, 2019). That gap still matters. Evidence for THC is deeper than evidence for CBD in many settings, and evidence for pharmaceutical preparations is often stronger than evidence for dispensary-style products, mixed formulations, or homemade edibles.
This article therefore takes a corrective stance. Cannabis pharmacokinetics is not settled into a few simple rules. It is route-dependent, formulation-dependent, dose-dependent, and person-dependent. Two products labeled with the same milligrams of THC or CBD can produce different peak plasma concentrations, different timing of onset, and different metabolite patterns. And even when concentrations are measured accurately, those numbers do not automatically map onto clinical effect.
What pharmacokinetics means for cannabinoids
Pharmacokinetics asks a plain question: what does the body do to a drug over time? The classic framework is absorption, distribution, metabolism, and excretion.
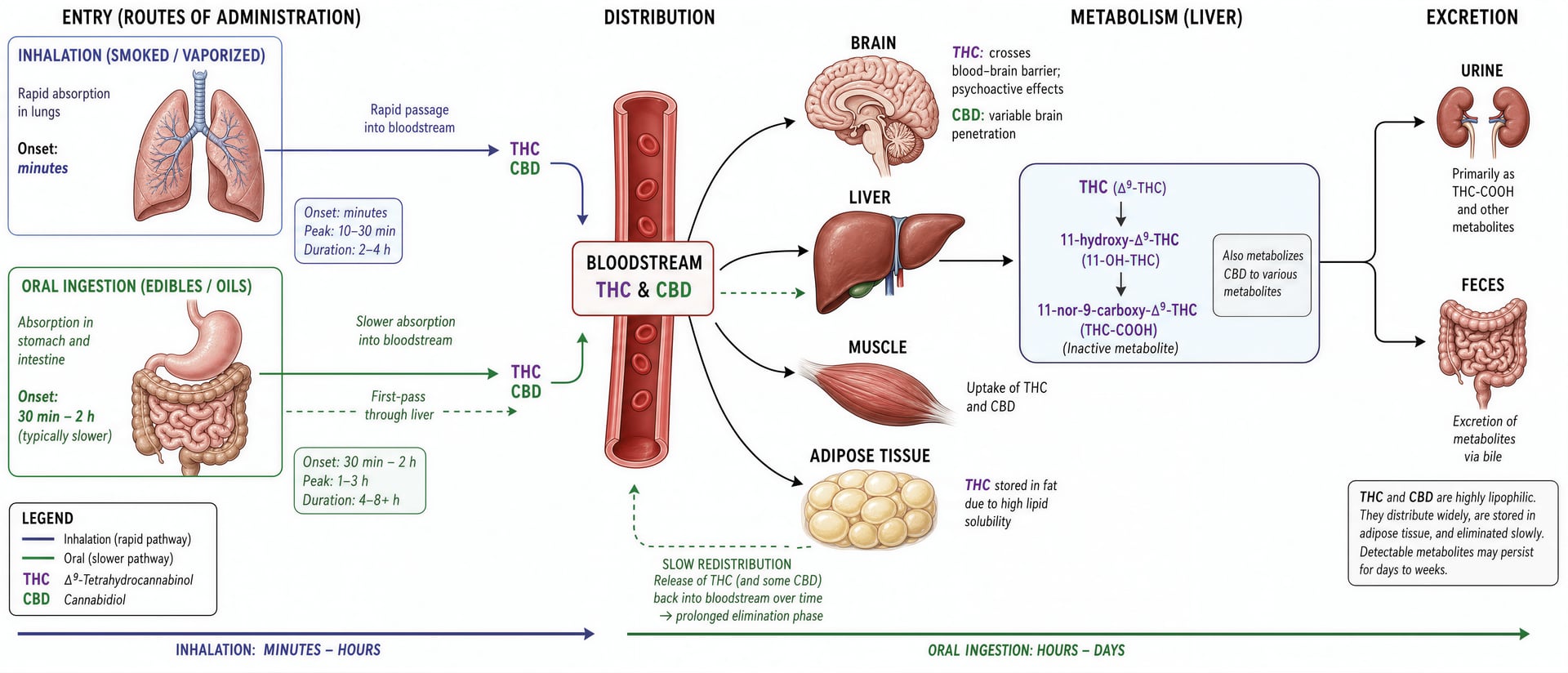
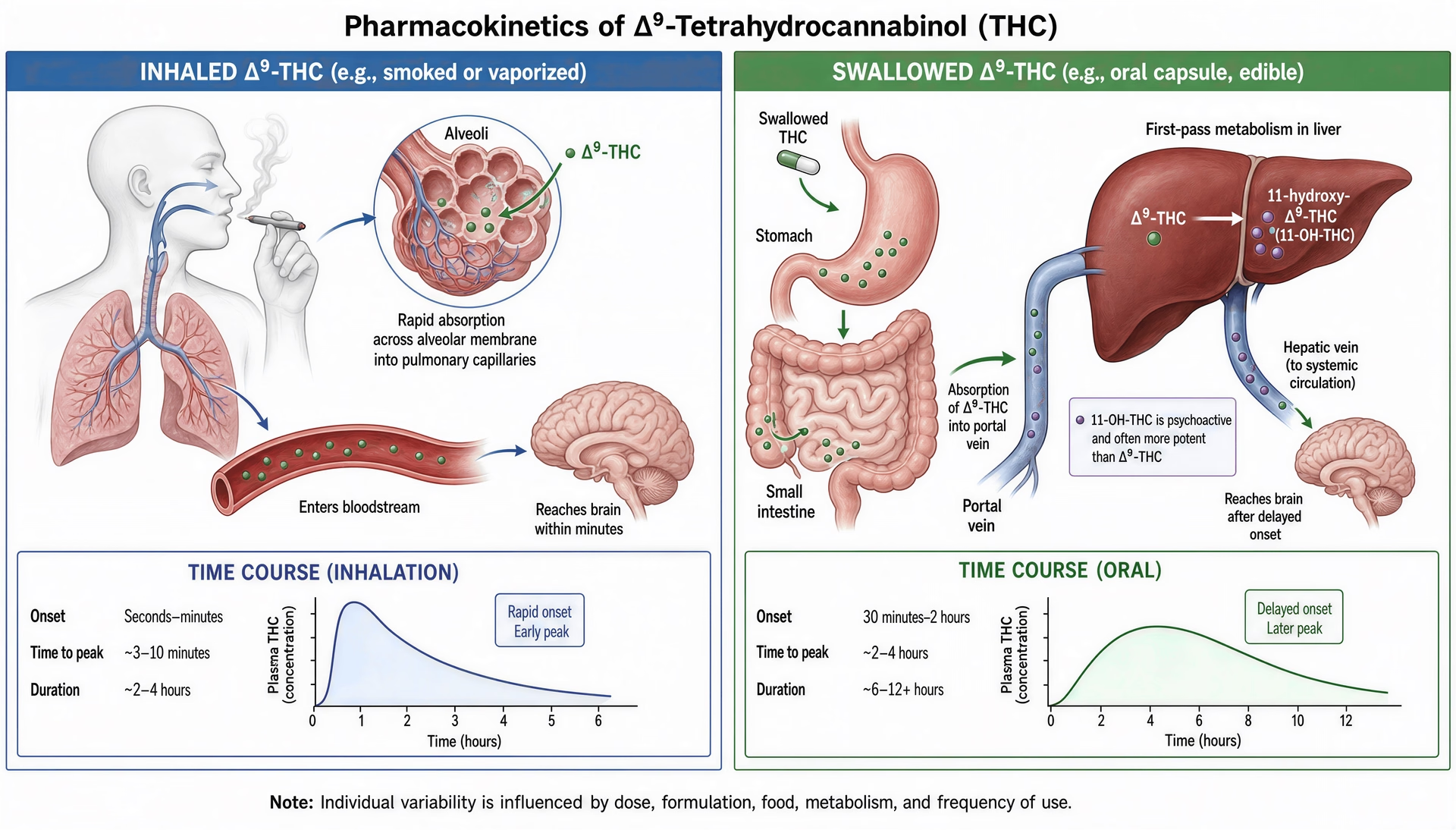
Absorption is how a cannabinoid gets from the product into the bloodstream. If THC is smoked or inhaled as an aerosol, it can cross the lungs quickly; NIDA notes that when marijuana is smoked, THC rapidly passes from the lungs into the blood and is then carried throughout the body, including the brain. If THC or CBD is swallowed, absorption is slower and less predictable because the compound has to move through the gut and then the liver first. NIDA gives the familiar oral timing estimate—effects usually begin after about 30 minutes to 1 hour—but that headline number hides major variation from food, formulation, and individual physiology.
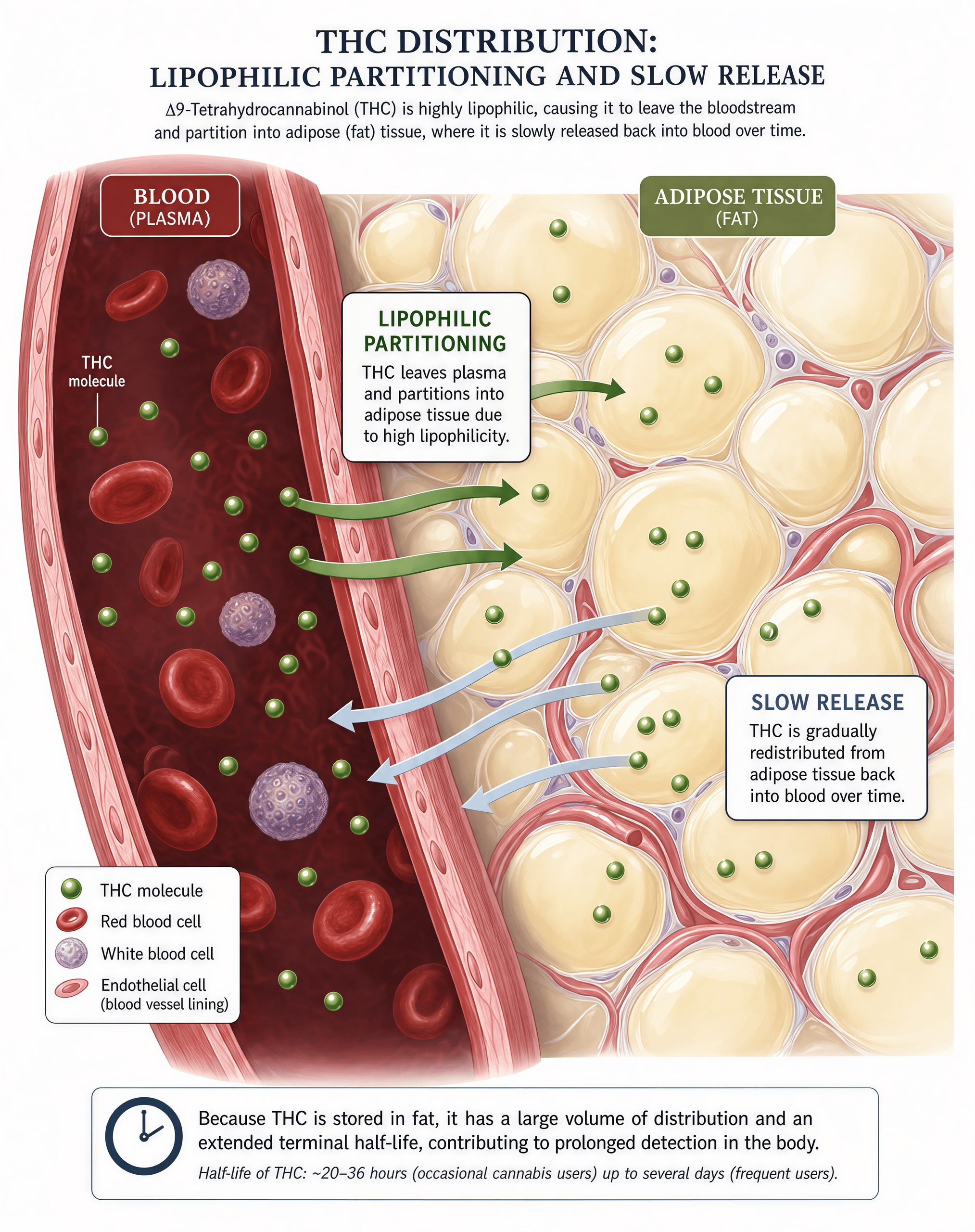
Distribution is where the compound goes once it is in circulation. Cannabinoids are highly lipophilic, which means they dissolve more readily in fat than in water. That matters because distribution is not limited to blood. THC and related compounds move into tissues, including adipose tissue, and that helps explain why blood levels can fall quickly even while metabolites remain detectable for much longer. The CDC makes this point in simple terms: THC is detectable in blood only for a short time, roughly 3 to 4 hours, while urine detection can last much longer because THC is stored in body fat and released gradually.
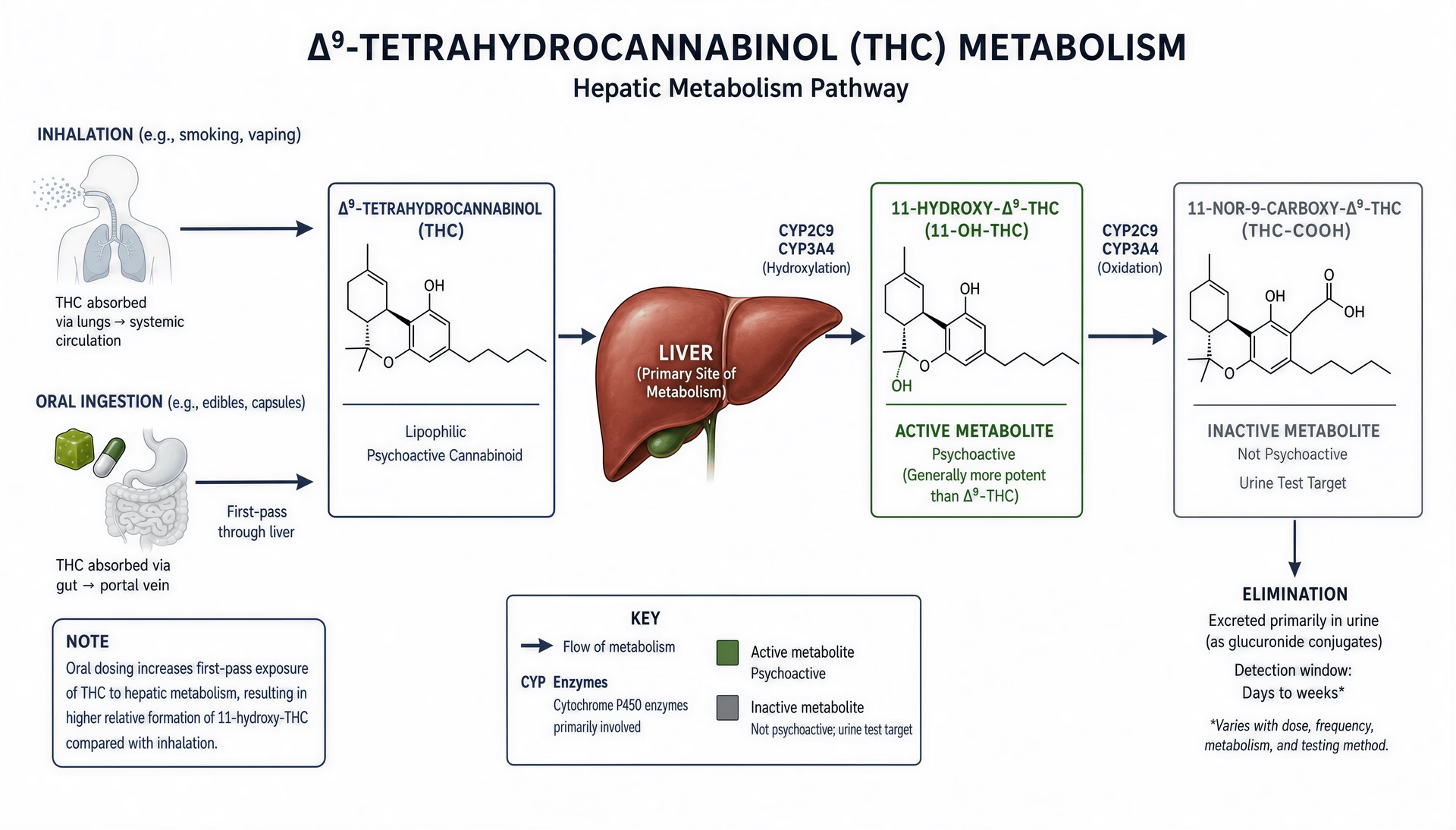
Metabolism is the chemical transformation of the parent compound into metabolites, mainly by liver enzymes. For THC, this is not a side detail. It changes the pharmacology. StatPearls notes that the major active metabolite of delta-9-tetrahydrocannabinol is 11-hydroxy-delta-9-THC, while the major inactive metabolite is 11-nor-9-carboxy-delta-9-THC. Oral THC tends to produce more first-pass metabolism than inhaled THC, so 11-hydroxy-THC often contributes more to systemic exposure after edibles. That is one reason an edible can feel different from inhaled cannabis even when the labeled THC amount appears similar.
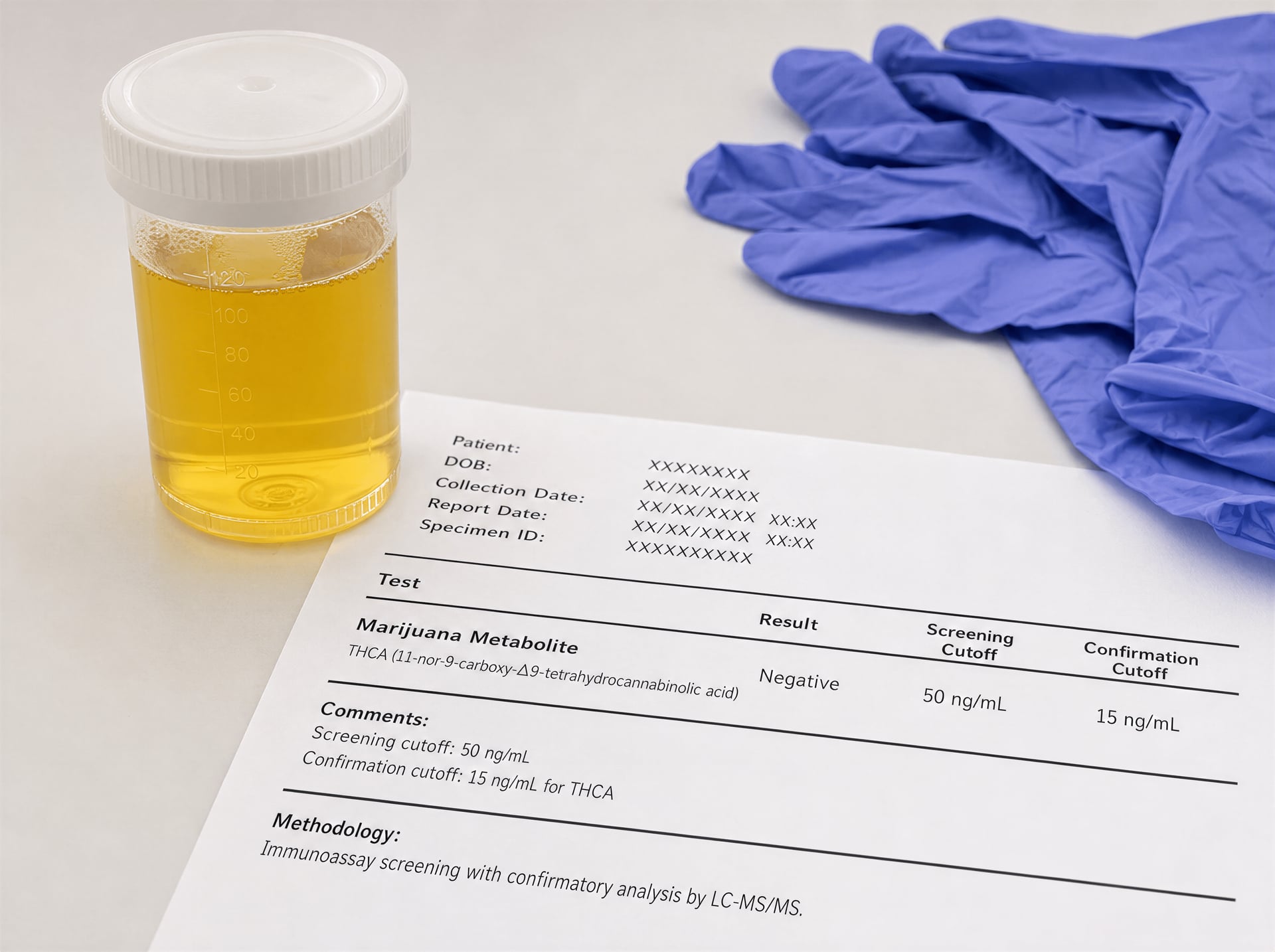
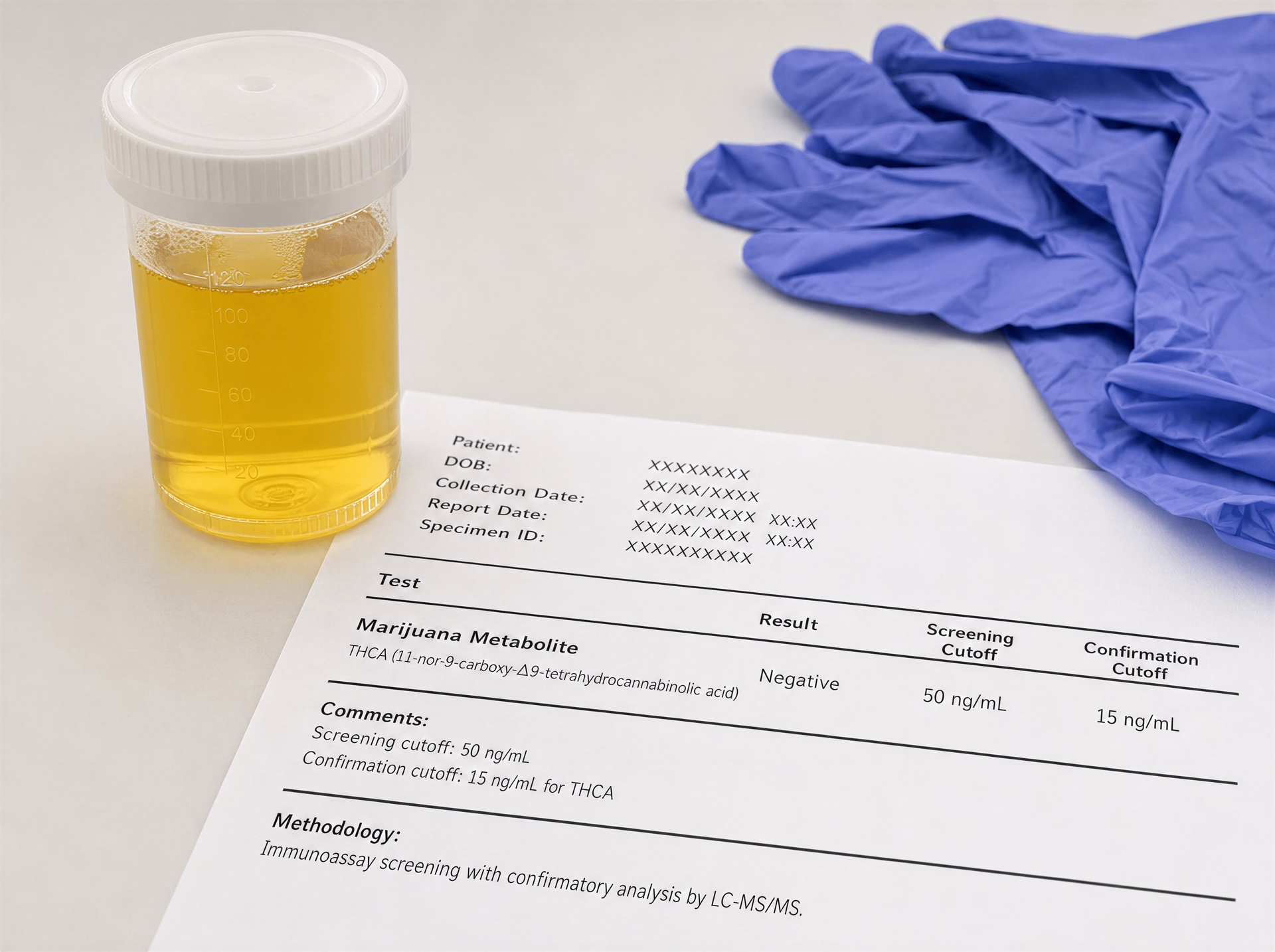
Excretion is how the body clears the parent drug and its metabolites, through urine, feces, and other routes over time. Here again, the popular story is too neat. A urine test is usually not detecting acute THC intoxication. Under SAMHSA’s 2024 federal workplace standards, a urine specimen screens positive for marijuana metabolite at 50 ng/mL and is confirmed positive at 15 ng/mL for THCA by GC/MS or LC/MS. That is a metabolite threshold, not a direct measure of current effect.
One more distinction prevents a lot of confusion: pharmacokinetics is not pharmacodynamics. Pharmacokinetics covers concentration over time in blood and tissues. Pharmacodynamics covers what those concentrations do at receptors and how they relate to effects such as analgesia, sedation, anxiety, tachycardia, or impairment. The two are related, but they are not interchangeable.
Why CBD research exposed major evidence gaps
CBD was a stress test for the field. The 2019 Nature Medicine feature captured an awkward reality: public adoption surged faster than the science. Researchers were still trying to pin down basic questions about cannabidiol handling in the body even while CBD was being added to oils, foods, tinctures, and wellness products. That should have ended the illusion that cannabinoid pharmacokinetics was already fully mapped.
Part of the problem was product heterogeneity. “CBD” in a purified oral solution is not the same as CBD in a lipid capsule, a vaporized extract, a beverage, or a full-spectrum oil with other cannabinoids and terpenes present. Another problem was that many early studies were small, used different analytical methods, or focused on narrowly defined formulations. The result was a literature with real findings but limited portability across product categories.
CBD also reminded researchers that low-bioavailability oral cannabinoids are hard to generalize about. Food effects can shift exposure sharply. Prescription cannabinoid products make this visible because they are studied under tighter conditions than most consumer products. The FDA labeling for oral dronabinol, a synthetic delta-9-THC formulation, reports peak plasma concentrations at about 2 to 4 hours and a terminal half-life of roughly 25 to 36 hours. Those figures come from a controlled medicine, not a brownie or gummy, yet they already show how much timing and persistence can diverge from the casual “edibles take an hour” simplification.
Why route, formulation, dose, and person all matter
Route matters first because it changes the path into circulation. Inhalation can produce rapid entry into blood. Oral ingestion sends cannabinoids through the digestive tract and liver, increasing delay and first-pass metabolism. The National Academies’ 2017 report synthesized this route dependence clearly: inhalation tends to produce faster onset and shorter duration than oral administration. But route is only the beginning.
Formulation changes absorption enough that equal labeled doses may not behave equally. A cannabinoid dissolved in oil, trapped in a capsule, suspended in a beverage, baked into food, or delivered as an oromucosal spray does not meet the body under the same conditions. Gastric emptying, bile secretion, particle size, excipients, and whether the product is taken with food can all shift Tmax, Cmax, and total exposure. Even pharmaceutical data show this instability, which means claims of precision for loosely regulated products should be treated cautiously.
Dose matters because cannabinoid kinetics are not always neatly proportional across the full dosing range. Higher doses may alter absorption dynamics, saturate parts of metabolism, or prolong the terminal phase as redistribution from fat becomes more relevant. Person matters because bodies differ. Age, sex, body fat, liver enzyme activity, genetics, prior cannabis exposure, co-administered drugs, and disease states can all change what happens after the same nominal dose.
That is why blood and urine findings are so easy to overread. Plasma concentration can miss the timing of peak effect, especially with oral products. Urine metabolite positivity can persist long after acute intoxication has passed. And respiratory route should not be discussed only in kinetic terms: the National Academies found substantial evidence linking cannabis smoking with worse respiratory symptoms and more frequent chronic bronchitis episodes, a reminder that route decisions affect both pharmacokinetics and health risk.
The short version is not “inhaled versus edible.” It is variability, at every step.
Absorption: how cannabinoids enter the body depends on route, formulation, and first-pass exposure
Absorption is where simple cannabis rules start to break down. “Smoking acts fast, edibles act slow” is directionally true, but it leaves out the mechanics that matter most: where the drug is absorbed, how much survives the trip, whether the liver transforms it before it reaches the rest of the body, and how the product itself was built. Those factors change not only timing but also which molecules circulate. That is a major reason oral THC can feel different from inhaled THC even when the labeled dose looks similar.
The evidence base is also less settled than many summaries imply. A 2019 Nature Medicine news feature on cannabidiol pointed out that researchers were still working out basic questions about CBD absorption and metabolism even as use surged. That should temper any claim that cannabinoid pharmacokinetics is a solved topic. It is not. Route matters. Formulation matters. Person-to-person variation matters.
Inhalation through smoking and vaporization
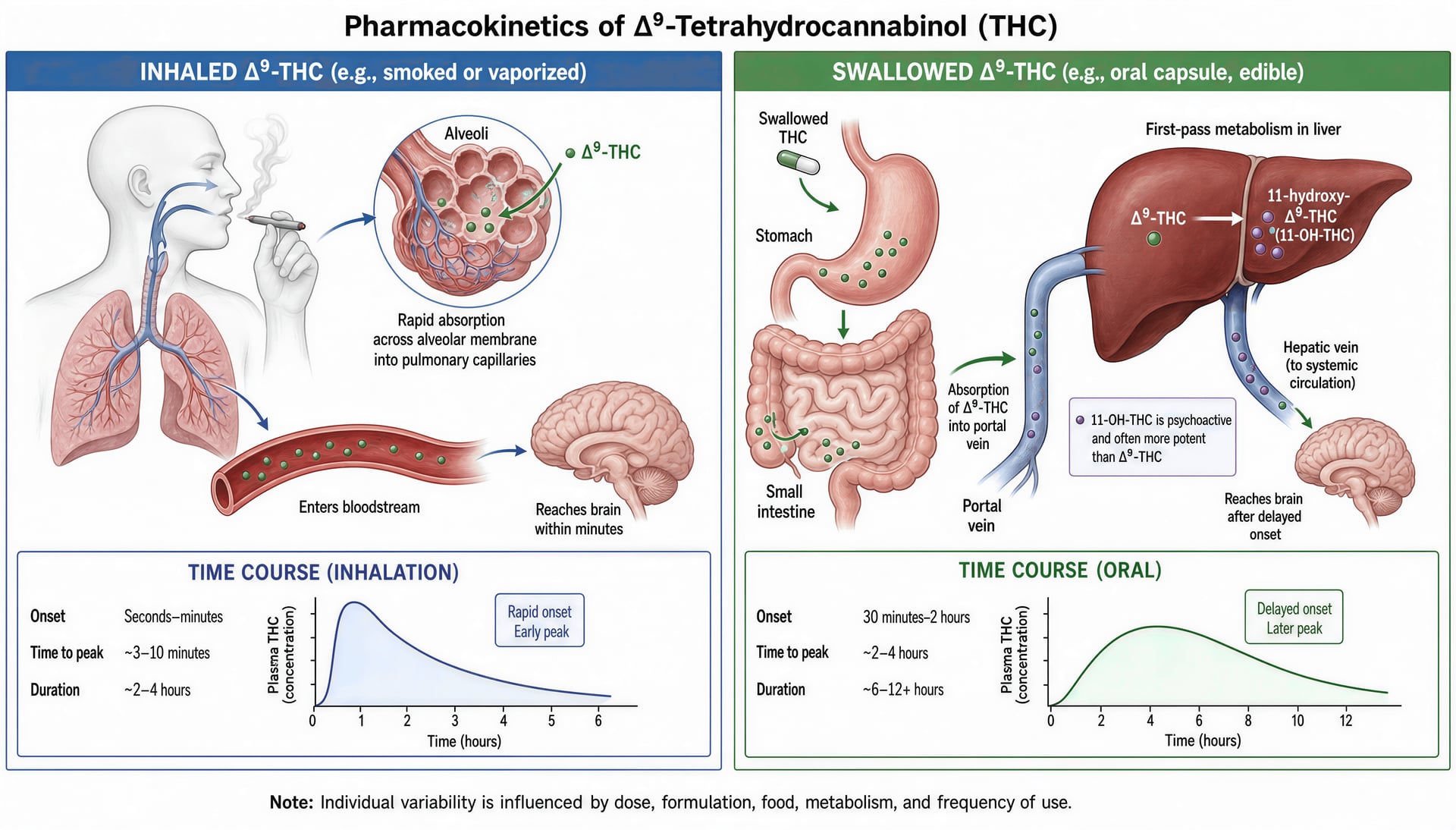
Inhalation is the fastest common route because the lung is an efficient transfer surface. NIDA states it plainly: when marijuana is smoked, THC “quickly passes from the lungs into the bloodstream,” and from there it is carried to organs throughout the body, including the brain. That one sentence captures the core pharmacokinetic advantage of inhalation. The drug does not need to survive gastric acidity, intestinal transit, or an initial pass through the liver before entering systemic circulation.
That is why effects can begin within minutes. The National Academies’ 2017 report draws the same route-based distinction, describing inhalation as a rapid-onset route compared with oral dosing. Yet even within inhalation, absorption is not a fixed quantity. A smoked joint, a high-powered vaporizer, and a metered medical inhalation system do not deliver cannabinoids in the same way. Puff duration, inhalation depth, breath-hold time, temperature, and combustion losses all change the amount that actually reaches the alveoli.
Smoking and vaporization also differ in what happens before absorption. Smoking involves combustion, which destroys part of the available THC and produces a complex aerosol that includes toxic byproducts. That matters clinically as well as pharmacokinetically, because a route can be fast and still come with tradeoffs. The National Academies found substantial evidence of a statistical association between cannabis smoking and worse respiratory symptoms and more frequent chronic bronchitis episodes. Vaporization may reduce exposure to some combustion products, but it does not erase dose variability or make pulmonary delivery pharmacokinetically uniform.
Another common mistake is treating rapid onset as equal to simple interpretation. Inhaled THC enters blood quickly, but blood concentrations can rise and fall faster than the experienced effects are often described in casual conversation. A person may have a high early plasma level shortly after smoking or vaping, then a sharp decline as THC distributes into tissues. So “fast in” does not mean “easy to read” when trying to connect a blood number to timing, intensity, or functional effect.
Oral ingestion, delayed onset, and first-pass metabolism
Oral cannabinoids follow a very different path. NIDA gives a hard reference point that is useful because it is concrete: if marijuana is consumed in foods or beverages, effects are delayed, “usually appearing after 30 minutes to 1 hour,” because the drug must first pass through the digestive system and liver before reaching the bloodstream. That statement is accurate, but it is only a starting point. In practice, onset can easily stretch beyond an hour, especially after a large mixed meal, with dense edible matrices, or with formulations that dissolve poorly.
First-pass metabolism is the central reason oral THC should not be treated as just a slower version of inhaled THC. After gastrointestinal absorption, portal blood carries THC to the liver before much of it reaches the rest of the body. There, hepatic enzymes convert part of the dose to 11-hydroxy-delta-9-THC, the major active metabolite identified in StatPearls, while 11-nor-9-carboxy-THC is the major inactive metabolite. This matters because oral dosing tends to produce greater relative exposure to 11-hydroxy-THC than inhalation does. That metabolite is psychoactive. So route changes the circulating mixture, not just the clock.
This is one reason the oral experience can be stronger, longer, or simply different than users expect from the same nominal milligram amount. A person who thinks “10 mg is 10 mg” is missing the pharmacology. Ten milligrams inhaled is not pharmacokinetically equivalent to ten milligrams swallowed.
The FDA labeling for dronabinol makes the timing problem even clearer. For oral dronabinol capsules, peak plasma concentrations are typically reached at 2 to 4 hours after administration. That figure is much later than the often-quoted 30-minute to 1-hour onset window, and the gap is important. Onset and peak are not the same thing. An edible may begin to be felt around an hour yet not reach peak blood concentrations until several hours later. People who redose too soon often do so inside that window of rising absorption.
Formulation further complicates oral exposure. Cannabinoids are highly lipophilic, so they dissolve poorly in water and behave differently depending on whether they are delivered in oils, baked goods, gelatin matrices, capsules, nanoemulsions, or other lipid-containing systems. A fatty meal can increase absorption of some oral cannabinoid products by improving solubilization and lymphatic transport, while a dry baked edible with inconsistent cannabinoid distribution may produce slower or less predictable uptake. Even pharmaceutical products show this variability. The FDA’s dronabinol labeling reports not only a 2-to-4-hour time to peak but also a terminal half-life of about 25 to 36 hours, underscoring that oral THC handling extends far beyond the first felt effect.
CBD adds another layer. The 2019 Nature Medicine feature highlighted how much remained uncertain about cannabidiol pharmacology despite widespread use. Oral CBD products vary enormously in absorption because formulation, coadministered food, and intestinal metabolism all matter. Casual claims that “CBD works in 20 minutes” or “CBD has high bioavailability” often rest on oversimplified or non-comparable data.
Oromucosal, sublingual, and other less-discussed routes
Oromucosal and sublingual delivery are often presented as a clean workaround for oral delay. The theory is sound: if THC or CBD is absorbed across the oral mucosa, some of the dose can enter systemic circulation without going straight through the gut and liver. That should reduce at least part of first-pass metabolism and may shorten onset compared with a swallowed edible.
But real-world exposure is usually mixed. Tinctures, sprays, dissolving strips, and lozenges are rarely absorbed entirely through the mouth. Some fraction is held long enough for transmucosal uptake; some is swallowed and handled like an oral dose. That means the resulting pharmacokinetic profile can contain an early component from mucosal absorption and a later component from gastrointestinal absorption. Users often interpret that as inconsistency when it is really a two-route delivery problem.
This is why sublingual products do not always behave as quickly as marketing language suggests. Saliva production, contact time, the concentration gradient across the mucosa, excipients, ethanol content, and the person’s technique all influence how much dose escapes swallowing. A spray directed at the buccal mucosa may produce faster initial absorption than a thick oil placed under the tongue and swallowed within seconds. The label route does not guarantee the actual route.
Other less common routes make the same point. Rectal administration, where studied, may partially reduce first-pass exposure depending on venous drainage, though published data are limited and product behavior is variable. Topical cannabinoids usually aim for local tissue exposure rather than substantial systemic absorption, while transdermal systems are designed specifically to move drug across the skin barrier over time. Those distinctions matter because “applied on the body” says almost nothing about systemic cannabinoid entry unless the formulation is built for that purpose.
Absorption, then, is not just about speed. It is about path. Lungs deliver cannabinoids rapidly to blood and brain. The gut delays entry and routes much of the dose through hepatic conversion, increasing exposure to 11-hydroxy-THC. Oromucosal products sit between those extremes, often only partly bypassing first-pass metabolism. Once route is combined with formulation, meal effects, and individual biology, the familiar quick rules stop being reliable.
Distribution: why cannabinoids spread quickly, accumulate in fat, and outlast their immediate effects
Distribution is the stage that often gets flattened into a misleading slogan. People hear that THC “hits fast” when inhaled and “lasts longer” when eaten, then assume the rest is simple. It is not. Once cannabinoids enter the bloodstream, they do not stay there in any stable, easily interpreted way. They move rapidly into well-perfused organs, partition into tissues with very different affinities, undergo ongoing exchange between blood and fat stores, and leave behind metabolites that can persist long after the felt effects have faded. That is why a blood number, by itself, tells much less than many public discussions suggest, and why a urine result is a marker of prior exposure rather than current effect.
Nature Medicine made this point indirectly in a 2019 news feature on cannabidiol research: even as CBD use surged, basic questions about absorption, distribution, and metabolism were still being worked out. That observation matters beyond CBD. It is a warning against treating cannabinoid pharmacokinetics as fully settled, especially across different routes, formulations, and patterns of use.
From bloodstream to brain and peripheral tissues
The first minutes after cannabinoids reach the blood are dominated by distribution, not elimination. NIDA states it plainly for smoked cannabis: THC quickly passes from the lungs into the bloodstream and is then carried to organs throughout the body, including the brain. That early movement is driven by perfusion. Organs receiving high blood flow, such as the brain, heart, lungs, and liver, are exposed first and most intensely. With inhalation, this process is fast enough that psychoactive effects can begin within minutes, because THC reaches the central nervous system before much metabolic conversion has occurred.
That early phase helps explain a common laboratory pattern. Blood THC concentrations can rise sharply, then fall sharply, even while effects are still present. The initial decline after a peak is often not proof that the drug has been “cleared.” Much of it reflects redistribution out of plasma and into tissues. Plasma is the transport medium, not the main storage site.
Route matters here. When a cannabinoid is inhaled, arterial blood leaving the lungs delivers parent THC to the brain quickly. When it is swallowed, absorption is slower and the liver intervenes before much of the dose reaches systemic circulation. NIDA notes that with cannabis consumed in foods or beverages, effects usually appear after 30 minutes to 1 hour because the drug must pass through the digestive system and liver first. That route changes not just timing but what is circulating. Oral exposure produces more first-pass metabolism, including more 11-hydroxy-THC, the major active metabolite identified in StatPearls, and that can alter both intensity and duration of effects.
Pharmaceutical data make the point concrete. The FDA labeling for oral dronabinol reports peak plasma concentrations at about 2 to 4 hours after dosing, far slower than inhaled THC. Yet even with that delayed peak, blood levels still do not provide a clean map of response, because distribution into tissues and ongoing metabolism continue while concentrations are changing. The body is not waiting politely for a single peak and decline.
Peripheral tissues matter too. Cannabinoids reach muscle, liver, adipose tissue, and other compartments that differ in blood flow and chemical affinity. CBD, THC, and related compounds are highly protein-bound and strongly lipophilic, so their movement is shaped not just by circulation but by where they “prefer” to partition. In practical terms, the brain is exposed early because of blood flow; fat becomes important later because of storage.
Lipophilicity, adipose storage, and redistribution
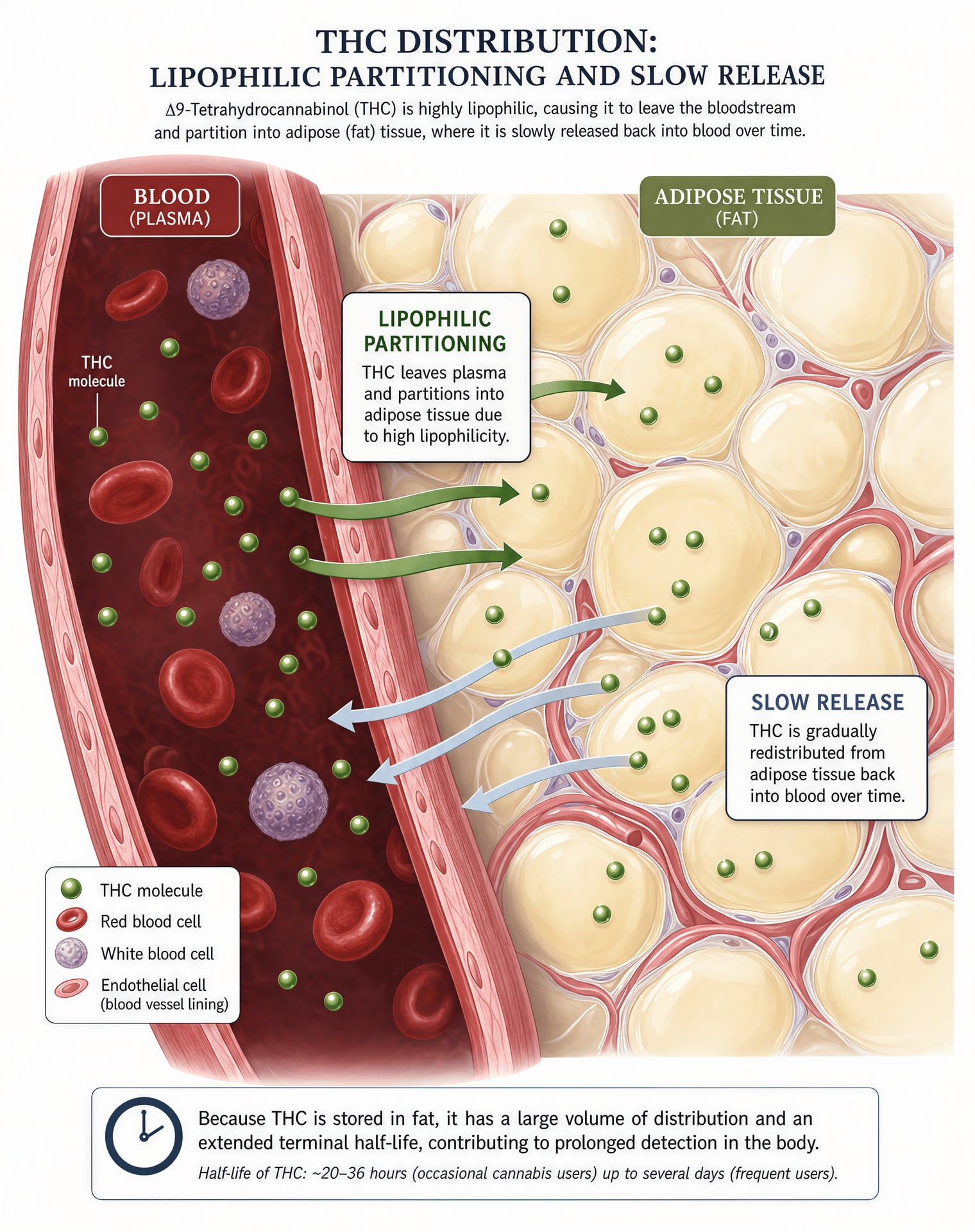
THC is highly lipophilic, and that property changes almost everything about its distribution. Lipophilic compounds dissolve far more readily in fats than in water, so they do not remain confined to the aqueous portion of blood. Instead, they partition into lipid-rich tissues, especially adipose tissue. CBD is also lipophilic, though the clinical implications remain less fully characterized than many casual summaries imply.
The CDC gives the public-facing version in simple language: THC is stored in body fat and slowly released. That single sentence explains why detection can outlast obvious intoxication by a wide margin. It also explains why the early drop in plasma THC after inhalation should not be mistaken for disappearance from the body. A substantial fraction has simply moved elsewhere.
Redistribution follows storage. As blood concentrations fall, cannabinoids stored in tissues can move back into circulation over time, though usually at low concentrations. This does not recreate the initial acute effect seen during rapid brain exposure, but it does prolong the pharmacokinetic tail. For oral dronabinol, the FDA lists a terminal half-life of about 25 to 36 hours. That figure reflects more than simple metabolic destruction. Tissue partitioning contributes to a long terminal phase because the drug is leaving storage compartments gradually while metabolism and excretion continue.
This is one reason detection-window claims are so unreliable when presented as fixed numbers. Two people can use similar amounts and show different persistence because their distribution kinetics differ. Body composition matters. A person with greater adipose mass may have a larger storage compartment for lipophilic cannabinoids. Frequency of use matters too. Repeated exposure can load tissue reservoirs more heavily than occasional use, changing both baseline concentrations and the pace of decline after stopping. Age can matter through shifts in body composition and organ function. Hepatic function matters because metabolism and redistribution are linked; if liver biotransformation slows, parent compounds and active metabolites may persist differently. Product chemistry matters as well. THC-dominant inhaled flower, oral THC in oil, an edible containing both THC and CBD, or a purified pharmaceutical capsule do not produce identical distribution profiles.
Even the matrix being tested changes what is being seen. Blood is a moving snapshot of parent drug and some metabolites. Urine mainly reflects excreted metabolites, especially 11-nor-9-carboxy-THC, the major inactive metabolite identified by StatPearls. Because adipose release can continue over time, metabolite production and excretion can continue after the psychoactive phase is over.
Why concentration does not map neatly onto impairment
This is the point most often mishandled in public discussion. A falling blood THC concentration does not mean cannabinoids have fully left the body. A positive urine test does not show current impairment. Those are different questions, and distribution is a major reason they come apart.
The CDC states that THC is detectable in blood only for a short time, about 3 to 4 hours, while urine testing can detect cannabis for much longer because THC is stored in body fat and slowly released. That statement should end the lazy claim that a positive urine test proves recent effect. Urine testing is built around metabolites, not real-time brain exposure. Under SAMHSA’s 2024 federal workplace standards, a urine specimen is reported positive for marijuana metabolite if the initial immunoassay screen is at or above 50 ng/mL and confirmatory testing is at or above 15 ng/mL for THCA. Those cutoffs are administrative thresholds for detecting prior exposure. They are not impairment thresholds.
Blood is not simple either. During the early post-inhalation period, THC can be high in blood because distribution to the brain is happening rapidly. Soon after, blood concentrations can fall steeply as the drug redistributes into tissues, even though the person may still be experiencing effects. Later, low blood concentrations may coexist with no meaningful acute effect at all, especially in frequent users with residual background levels. The same measured concentration can therefore mean different things in different people.
That variation is not a minor footnote. It is central. Frequency of use changes tissue loading. Body fat changes storage capacity. Age and liver function can change both tissue handling and metabolism. Formulation can change which cannabinoids and metabolites dominate systemic exposure. Oral products, for instance, may produce more 11-hydroxy-THC relative to inhaled products, and that can alter the relationship between parent THC concentration and observed effect.
The practical result is that acute psychoactive effects can recede well before metabolites disappear from urine, and measurable cannabinoids or metabolites can persist after obvious impairment has ended. Distribution is the bridge between those facts. Once THC and related cannabinoids leave plasma, enter the brain quickly, settle into fat, and then leak back out slowly, any claim of a single exact detection window starts to look less like science and more like oversimplification.
Metabolism: liver enzymes, active metabolites, and the special case of CBD
Metabolism is where many simplified cannabis explanations fall apart. “THC is THC” sounds neat, but it is pharmacokinetically false. What reaches the bloodstream is not always what reaches tissues later, and what produces effects after an oral dose is shaped heavily by what the liver does before much parent compound ever enters systemic circulation. For THC especially, route of administration changes not just how fast effects start, but which molecules dominate exposure. That matters for clinical effects, adverse effects, and interpretation of blood or urine findings.
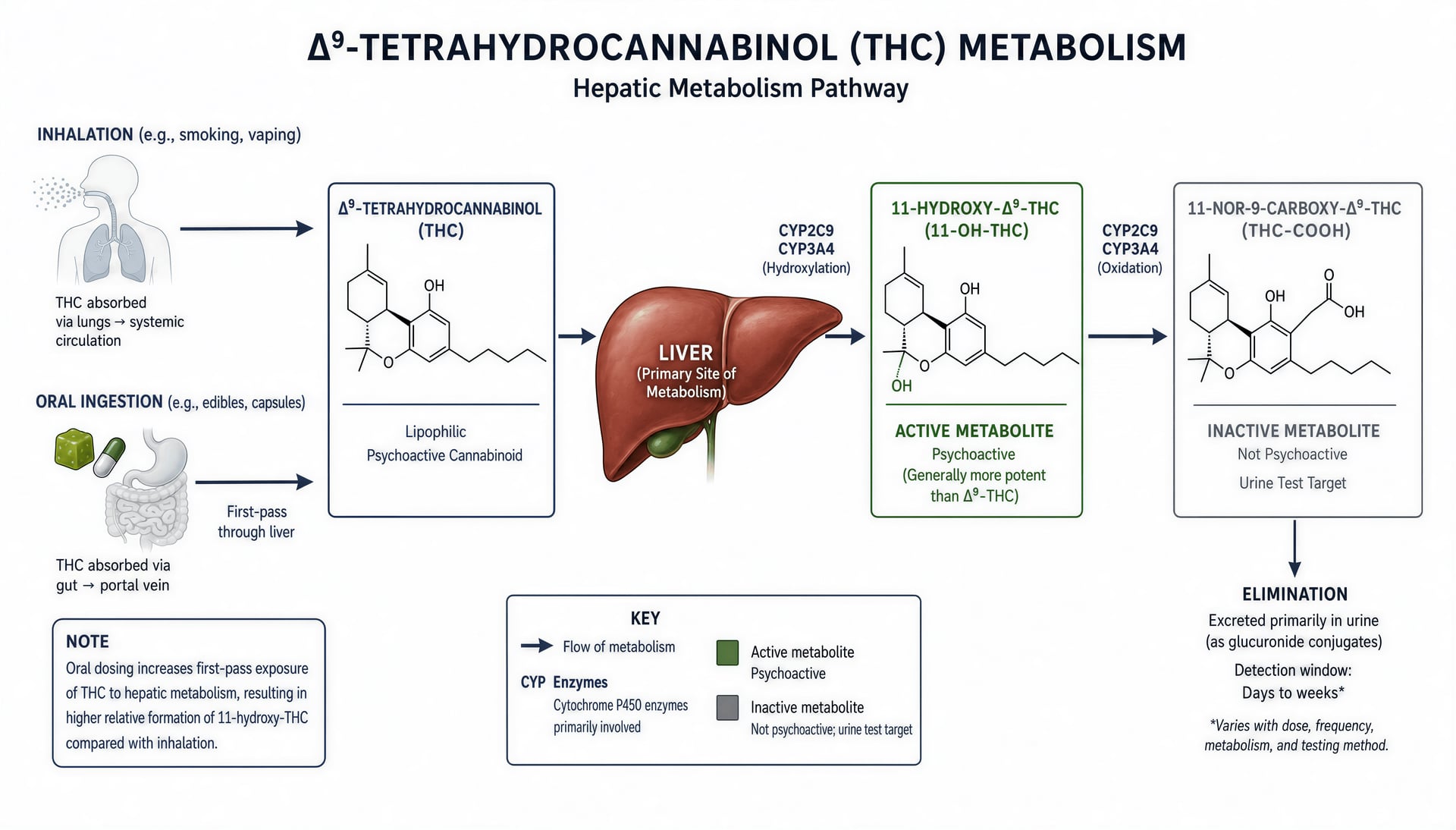
StatPearls, published through the NCBI Bookshelf, states the core pathway plainly: the major active metabolite of delta-9-tetrahydrocannabinol is 11-hydroxy-delta-9-THC, and the major inactive metabolite is 11-nor-9-carboxy-delta-9-THC. Those two compounds explain a great deal of the confusion around oral cannabis, intoxication timing, and drug testing.
THC biotransformation to 11-hydroxy-THC and THC-COOH
After THC enters the body, hepatic metabolism converts part of the parent drug into 11-hydroxy-THC, often written 11-OH-THC. This is not a trivial breakdown product. It is the principal active metabolite, meaning it contributes to pharmacologic effects rather than merely marking that exposure happened. The next major step is oxidation to 11-nor-9-carboxy-THC, usually abbreviated THC-COOH, which is considered the major inactive metabolite. That distinction—active 11-OH-THC versus inactive THC-COOH—is basic to understanding why route matters so much.
With inhalation, THC moves rapidly from the lungs into blood, as NIDA notes, and reaches the brain before a large fraction has been processed by the liver. Metabolism still occurs, of course, but first-pass conversion is limited because the drug does not initially travel from the gut straight to the portal circulation and then through the liver. Oral dosing is different. NIDA’s 2024 summary says effects from foods or beverages are usually delayed by 30 minutes to 1 hour because the drug must pass through the digestive system and liver before reaching the bloodstream. That “and liver” part does a lot of work. It means more parent THC is converted during first pass, shifting exposure toward 11-hydroxy-THC before systemic circulation is fully established.
That is one reason oral THC can feel different from inhaled THC even when the nominal milligram amount appears similar. It is not just a slower version of the same curve. It is a different metabolite profile. Oral products often produce relatively greater exposure to 11-hydroxy-THC, and because 11-hydroxy-THC is active, this can amplify or reshape the experience compared with inhalation. Readers are often told only that edibles are delayed. The stronger point is that they are metabolically reweighted.
Pharmaceutical data make this easier to grasp than lifestyle writing usually does. The FDA labeling for oral dronabinol reports peak plasma concentrations at about 2 to 4 hours after administration, with a terminal half-life of roughly 25 to 36 hours. Dronabinol is not the same as every edible sold in the broader market, but it shows what an oral THC formulation can do under regulated conditions: slow rise, substantial hepatic processing, and persistence well beyond the onset window. Once that framework is understood, the leap from “delayed onset” to “different metabolite exposure” becomes unavoidable.
THC-COOH then enters the story not as the driver of acute effects, but as the main biomarker of prior THC metabolism. This is the metabolite central to urine testing. SAMHSA’s 2024 mandatory federal workplace testing cutoffs are explicit: an initial immunoassay screen is positive at or above 50 ng/mL, and confirmatory GC/MS or LC/MS testing is positive at or above 15 ng/mL for THCA, meaning the carboxylated metabolite target used in cannabis urine testing. That is why a positive urine result does not establish current intoxication. It shows that THC was metabolized and that metabolites remain present above threshold. The CDC makes the same practical point from a public health angle: THC is detectable in blood only for a short time, about 3 to 4 hours, while urine detection lasts much longer because THC is stored in body fat and slowly released. Metabolism and distribution are inseparable here. A metabolite-based test is reporting biochemical history, not a clean timestamp of impairment.
Cytochrome P450 pathways and interaction risk
The practical clinical issue is not memorizing every enzyme label. It is recognizing that cannabinoids pass through hepatic enzyme systems that also process many common prescribed drugs. When two substances depend on overlapping pathways, exposure can change in both directions. One drug can raise cannabinoid levels by slowing metabolism. A cannabinoid can raise the level of another drug by inhibiting its clearance. Sometimes the reverse happens if metabolic activity is increased. The point is interaction risk, not enzyme trivia.
For THC, first-pass metabolism means that oral products are especially exposed to this problem. If a patient takes a medication that reduces activity of the relevant hepatic pathways, more parent THC or more active metabolite may remain in circulation for longer, potentially intensifying effects or adverse reactions. If the medication induces metabolism, exposure may shift the other way. The same logic applies to prescribed cannabinoid medicines such as dronabinol, and it applies even more strongly when people combine cannabinoid products with other central nervous system drugs, antiseizure drugs, anticoagulants, or sedatives. Not every combination produces a clinically important change, but enough do that the principle should be treated seriously.
This is also where product type matters. Whole-plant preparations, purified isolates, and approved pharmaceuticals are not metabolically interchangeable simply because a label highlights one cannabinoid. A product rich in THC but also containing CBD and minor cannabinoids can behave differently from a purified THC capsule, not only because absorption differs, but because co-administered cannabinoids may alter enzyme activity, intestinal handling, or the fraction of drug available for first-pass conversion. Formulation matters too. Oils, capsules, baked products, beverages, and inhaled aerosols can send the same nominal cannabinoid dose into very different metabolic conditions.
So the clean story many readers learn—“THC enters, then leaves”—misses the central pharmacology. It enters, is transformed into active and inactive metabolites, is affected by route and formulation, and can in turn affect the handling of other drugs.
Why CBD metabolism remains an active research problem
CBD is often described as simpler than THC because it is non-intoxicating. That description is socially convenient and pharmacokinetically misleading. Non-intoxicating does not mean metabolically simple. CBD absorption is variable, oral bioavailability is inconsistent, food effects can be large, and hepatic metabolism creates real interaction potential. The literature has been catching up to mass use rather than guiding it from the start.
A 2019 Nature Medicine news feature made that gap unusually clear. As CBD use expanded rapidly across clinical, consumer, and wellness settings, researchers were still trying to pin down its absorption, distribution, and metabolism. That is not a minor footnote. It means public familiarity outran the evidence base. People spoke about CBD as if its pharmacology were settled, while investigators were still working through basic questions of exposure, metabolite patterns, dose scaling, and interaction liability.
The research problem exists for several reasons. First, CBD products vary widely in formulation. Oral oils, capsules, sublingual preparations, vaporized products, and prescription formulations do not yield the same concentrations over time. Second, CBD is metabolically active in the liver and can affect the same broad enzyme systems that handle other drugs. That creates a bidirectional interaction issue much like THC, but often with greater clinical attention because CBD is frequently used by people taking chronic medications, including antiseizure therapies. Third, many studies are not directly comparable because they use different doses, different formulations, fed versus fasted conditions, and different analytical methods.
Whole-plant products complicate the picture further. A CBD-dominant extract is not the same thing as purified cannabidiol. Small amounts of THC, terpenes, and minor cannabinoids may alter absorption, first-pass handling, or enzyme inhibition patterns. Even when CBD is the main named compound, the metabolic outcome may differ because the matrix differs. Pharmaceutical cannabidiol products, by contrast, offer tighter control over composition, which helps define kinetics but does not erase interaction concerns.
That is the key position the evidence supports: CBD should not be treated as pharmacokinetically straightforward just because it does not produce the classic intoxicating effects associated with THC. Its metabolism is active, formulation-sensitive, and clinically relevant. Rising use came first. Clear metabolic answers have arrived more slowly.
Excretion and detection: how cannabinoids leave the body, and what drug tests do and do not show
Excretion is the last step in the pharmacokinetic story, but it does not begin only when someone stops feeling effects. By the time cannabinoids are leaving the body in measurable amounts, they have already been absorbed, distributed into tissues, transformed by metabolism, and in many cases redistributed out of fat stores back into blood. That sequence matters because drug testing is often treated as if it captures one clear event—recent use, current effect, or “being impaired”—when it usually captures something much messier: the lingering chemical aftermath of prior exposure.
That caution is especially important because the evidence base is still incomplete in places. A 2019 Nature Medicine news feature on cannabidiol pointed out that even as CBD use expanded rapidly, researchers were still working out basic questions about absorption, distribution, and metabolism. The same warning applies to interpretation. Popular rules are too simple. Route, dose, frequency of use, body composition, and test type all change what a positive result means.
Urinary and fecal elimination at a high level
Cannabinoids do not leave the body mainly as unchanged THC. After intake, delta-9-tetrahydrocannabinol is metabolized into downstream compounds, including the active metabolite 11-hydroxy-delta-9-THC and the major inactive metabolite 11-nor-9-carboxy-delta-9-THC, often abbreviated THC-COOH or THCA in drug-testing contexts. StatPearls, updated in 2024, identifies those two metabolites as the key products to know. That distinction matters because urine testing is generally looking for metabolite evidence, not for the parent THC molecule that produced acute psychoactive effects.
At a high level, cannabinoid metabolites are excreted through both urine and feces over time. The exact split depends on the compound, route of administration, formulation, and study design, and the available sources here do not justify pretending there is one fixed proportion that applies to every case. What can be said with confidence is that excretion is prolonged because cannabinoids are highly lipophilic. They do not remain confined to blood. NIDA’s 2024 overview explains that after smoking, THC rapidly moves from the lungs into the bloodstream and is then carried to organs throughout the body, including the brain. From there, distribution continues into other tissues, including adipose tissue.
That fat storage is central to long detection windows. The CDC states in 2024 that THC can be detected in blood only for a short time—about 3 to 4 hours—but urine testing can remain positive much longer because THC is stored in body fat and slowly released. That is the key frame for excretion: the body is not clearing one simple bolus from a single compartment. It is clearing metabolites while parent cannabinoids and related compounds can continue to redistribute from tissue stores. In a person who uses frequently, that slow release can keep feeding the metabolic and excretory pipeline long after obvious intoxication has ended.
Oral exposure can complicate this further. NIDA notes that when cannabis is consumed in foods or beverages, effects are delayed, usually appearing after 30 minutes to 1 hour, because the material must pass through the digestive system and liver before reaching systemic circulation. Oral cannabinoids undergo substantial first-pass metabolism, which changes which compounds circulate and for how long. The FDA labeling for oral dronabinol, a pharmaceutical delta-9-THC product, reports peak plasma concentrations at roughly 2 to 4 hours and a terminal half-life of about 25 to 36 hours. That is not a direct template for every edible on the market, but it does show why simplistic claims about “how long cannabis stays in your system” are poor science. Different formulations create different exposure curves, and excretion follows those curves.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Urine testing cutoffs and metabolite detection
Federal workplace urine testing does not ask whether any trace amount is present. It uses defined administrative thresholds. SAMHSA’s 2024 cutoff table states that for marijuana metabolites, the initial immunoassay screen is positive at 50 ng/mL, and the confirmatory test is positive at 15 ng/mL for THCA by GC/MS or LC/MS. Those numbers are widely cited, but they are often misunderstood.
First, a cutoff is not a biological boundary between “affected” and “unaffected.” It is a program rule for classifying a specimen. A urine sample with 49 ng/mL on the screening assay is not magically pharmacologically different from one with 50 ng/mL. One falls below the reporting threshold; the other triggers further action. The confirmatory threshold of 15 ng/mL serves a different purpose: once a specimen screens positive, a more specific analytical method verifies the presence of the target metabolite at or above that level. This system is about standardized testing and false-positive control, not measuring real-time drug effect.
Second, the analyte matters. Urine marijuana tests generally target THC-COOH, the inactive carboxy metabolite, rather than active THC in blood. That means the test is asking, in effect, whether the person has metabolized THC and is excreting its byproducts. It does not directly indicate when the cannabis was used, how much was used, what route was used, or whether the person is currently experiencing impairment.
Third, concentration in urine is shaped by more than dose. Hydration status, urine dilution, timing since last use, frequency of use, body fat, and individual metabolism all affect whether a result lands above or below a cutoff. A chronic user may continue producing positive urine specimens because previously stored cannabinoids are still being released and metabolized. A single low dose taken long before testing may produce a very different pattern. The same positive result category can therefore represent very different exposure histories.
Why detection is not the same as intoxication
This is the point most public discussion gets wrong. Detection means a test found a compound or metabolite above its reporting threshold. Intoxication refers to current psychoactive effect. Those are not interchangeable.
The CDC’s 2024 explanation draws the clearest line: THC is detectable in blood for only about 3 to 4 hours, while urine can remain positive much longer because of storage in body fat and slow release. Even that blood figure should not be overread as a universal impairment window, but it does show the mismatch between test types. Blood THC speaks, imperfectly, to recent exposure. Urine metabolites speak to prior exposure over a broader time frame. A positive urine test therefore cannot establish that someone was acutely impaired at the time the sample was collected, let alone at some earlier event such as a workplace incident or traffic stop.
Frequent use makes the problem worse. With repeated exposure, lipophilic cannabinoids accumulate in adipose tissue and other compartments, then re-enter circulation gradually. The person may feel fully sober while urine still contains enough THC-COOH to exceed SAMHSA’s 50 ng/mL screen and 15 ng/mL confirmation thresholds. That is not an edge case. It is one of the basic consequences of cannabinoid distribution and slow elimination.
The same logic applies when people compare routes too casually. Inhaled THC reaches blood fast. Oral THC reaches peak later and produces more first-pass metabolite formation, including 11-hydroxy-THC, which can contribute strongly to effects. Yet once testing shifts from blood parent compound to urine metabolite, those route-specific differences are blurred into a broader record of past metabolism. That is why urine testing is useful for documenting exposure but weak for proving current effect.
A defensible position, based on the CDC, SAMHSA, NIDA, FDA labeling, and standard pharmacology sources, is this: urine drug tests for cannabis are exposure tests, not impairment tests. They can show that cannabinoid metabolites were present above a chosen threshold. They cannot, by themselves, show that the person was intoxicated, unsafe, or impaired when the sample was taken. Any claim stronger than that goes beyond what the pharmacokinetics support.
Clinical and public-health implications: dosing, delayed effects, adverse reactions, and why PK literacy matters
Cannabis pharmacokinetics becomes most important at the exact point where popular advice usually becomes least precise: when someone is deciding whether to take more, when an emergency clinician is trying to judge recent exposure, when a workplace drug test is interpreted as if it proves current impairment, or when a policymaker writes rules that ignore route, formulation, and timing. The basic distinction between inhaled and oral products is real, but it is only the start. NIDA states that when cannabis is smoked, THC moves quickly from the lungs into the bloodstream, while effects from foods or beverages are delayed, usually appearing after 30 minutes to 1 hour because the drug must pass through the digestive tract and liver first (NIDA, 2024). That delay is not just a trivia fact. It is a setup for dosing errors, adverse reactions, and bad public messaging.
Why delayed oral onset leads to accidental overconsumption
The classic edible problem is not simply “edibles are stronger.” It is that oral dosing creates a long window in which the person may feel little or nothing and incorrectly assume the first dose was too small. That assumption often triggers a second dose before the first has reached full effect. By the time both doses are absorbed and first-pass metabolism has generated active metabolites, the total exposure may be far higher than intended.
The liver matters here. Oral THC does not enter systemic circulation in the same pattern as inhaled THC. First-pass metabolism increases production of 11-hydroxy-delta-9-THC, an active metabolite identified in StatPearls as the major active metabolite of delta-9-THC, while 11-nor-9-carboxy-delta-9-THC is the major inactive metabolite (StatPearls, 2024). That means route changes not only speed, but the composition of what circulates. A person comparing an edible to smoking is not merely comparing “slow” versus “fast.” They are comparing different metabolic paths and a different time course of effects.
Pharmaceutical data make this concrete. The FDA labeling for oral dronabinol reports peak plasma concentrations at about 2 to 4 hours after dosing and a terminal half-life of roughly 25 to 36 hours. Those numbers are for a standardized oral THC medicine, not a loosely described homemade edible, and even there the peak is far later than many people expect. If someone redoses at 45 minutes because “nothing happened,” they may still be well before peak exposure from dose one.
This is why public education that stops at “wait for it” is too thin. People need a practical rule tied to PK reality: delayed onset does not mean failed dose. It may mean absorption is still unfolding. The adverse outcomes that follow are often not mysterious toxicity in the dramatic sense, but severe intoxication: panic, vomiting, confusion, marked sedation, tachycardia, impaired coordination, or paranoia. Those reactions become more likely when multiple oral doses stack during the delay period. Children are a separate concern because edible products can be mistaken for regular food; the same PK delay can complicate recognition of what happened.
Respiratory route matters beyond pharmacokinetics
Fast onset by inhalation is often framed as an advantage because it lets the user titrate effects more quickly. That part is true. A person inhaling cannabis usually feels effects within minutes, which reduces the incentive to keep redosing blindly. But PK speed should not be confused with overall safety.
The National Academies report from 2017 found substantial evidence of a statistical association between cannabis smoking and worse respiratory symptoms and more frequent chronic bronchitis episodes. That finding matters because it separates two questions that are often blurred together. One question is how quickly THC reaches blood and brain. Another is what the route does to the lungs and airways over time. A route can offer faster feedback while still carrying pulmonary costs.
That distinction has clinical value. If a patient says smoking “works better” because it acts faster, the clinician should not answer only in PK terms. The response also has to address cough, sputum production, wheeze, and chronic bronchitis symptoms. Route choice is not a simple trade between convenience and speed. It changes organ exposure in ways that matter outside intoxication.
What patients, clinicians, and policymakers often miss
The first thing often missed is that toxicology results answer narrower questions than people assume. The CDC notes that THC is detectable in blood only for a short time, around 3 to 4 hours, while urine detection lasts much longer because THC is stored in body fat and slowly released (CDC, 2024). So a urine positive does not mean a person is acutely impaired. It usually means prior exposure. Under SAMHSA’s 2024 federal workplace standards, a urine specimen is positive for marijuana metabolite at an immunoassay cutoff of 50 ng/mL and a confirmatory cutoff of 15 ng/mL for THCA. Those are metabolite thresholds, not impairment thresholds.
The second thing missed is that route-specific history is mandatory for good clinical assessment. Asking only “do you use cannabis?” is weak history-taking. Clinicians need to know inhaled versus oral, product type, dose if known, time of last use, frequency, and whether CBD products are involved. They also need a medication review. Cannabinoids, especially orally administered products subject to hepatic metabolism, can interact with other drugs through enzyme effects and competition. That issue remains unsettled enough that the uncertainty itself is clinically relevant.
Nature Medicine highlighted this problem in 2019, reporting that even as CBD use surged, researchers were still trying to map its absorption, distribution, and metabolism. That should change how confident anyone sounds. If CBD, one of the most widely discussed cannabinoids, still has major PK gaps under active study, then claims that cannabis PK is already fully mapped are overstated. This is not an isolated CBD oddity. It reflects a broader challenge: cannabinoid disposition depends on route, matrix, dose, repeated use, body composition, and co-medications.
PK literacy matters because medicine safety, emergency triage, workplace policy, and public education all depend on it. Without that literacy, delayed oral onset gets mistaken for underdosing, positive urine tests get mistaken for present impairment, and fast inhaled onset gets mistaken for route safety overall. Cannabis pharmacokinetics is still a moving target, and the continuing effort to sort out CBD metabolism is one visible sign of that larger unfinished scientific job.